

Report 58: Histopathology Series Part 2 – “Autopsies Reveal Medical Atrocities of Genetic Therapies Being Used Against a Respiratory Virus”
This report is a follow-up to “Report 56: Autopsies Reveal Medical Atrocities of Genetic Therapies Being Used Against a Respiratory Virus” and offers critical additional analysis.
Histopathological reevaluation of serious adverse events and deaths following COVID-19 vaccination
Professor Arne Burkhardt
Pathologist
Reutlingen, Germany
Professor Dr. Arne Burkhardt gave an update on his series of autopsy and biopsy cases associated with Spike associated gene therapy entitled “Histopathological reevaluation of serious adverse events and deaths following COVID-19 vaccination” at the January 2023 Pandemic Strategies: Lessons and Strategies conference in Stockholm Sweden, presented by the Swedish physician group Läkaruppropet. (The Doctors’ Call) https://lakaruppropet.se/ [Note: A rough draft was prepared using voice recognition then was edited for clarity with an effort to retain Professor Dr. Burkhardt’s original meaning. The text was then added to the presentation graphics. Text in italics has been added by the current author.]
Arne Burkhardt, Professor and M.D. of Pathology studied Medicine at the Universities of Kiel, Munich and Heidelberg. He trained in Pathology at the Universities of Heidelberg and Hamburg (1970 -1979) and became Professor of Pathology at the Universities of Hamburg (1979) and Tübingen (1991). He holds a position as an Extraordinarius Emeritus for General and Special Pathology at the University of Bern, Switzerland, and has been practicing as a pathologist in his own laboratory since 2008. Dr. Burkhardt has held guest professorships in numerous universities in the United States (Harvard, Brookhaven), Japan (Nihon), South Korea, and Europe. He has authored more than 150 original publications in international and German medical journals and contributed to textbooks in German, English, and Japanese.
Summary
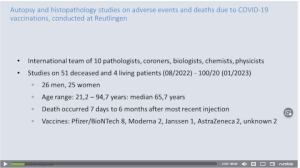
The Burkhardt Group (TBG) now consists of a 10-member international research team of pathologists, coroners, biologists, chemists and physicists.
TBG now has 100 autopsy and 20 biopsy cases in various stages of analysis, 51 of which are the subject of this report.
There were 26 men and 25 women; ages ranged from 21 to 94.
Death occurred from seven days to six months after the last injection of Spike-mediated gene therapy. The larger series had one case in which death occurred eight months after the last gene therapy injection.
The deceased received Spike-inducing drugs from four manufacturers: Janssen/Johnson and Johnson, Pfizer/BioNTech, Moderna and AstraZeneca.
Initial autopsy reports listed cause of death as or “natural” or uncertain in 49/51 cases.
Evaluation consisted of Histology, Special Stains, Immunochemistry, and Advanced physicochemical methods.
Forensic autopsy disclosed that the cause of death at a highly likely or likely level of probability (to a reasonable degree of medical probability) was from Spike-inducing gene therapy products in 80% of cases.
Findings:
I. General Lesions affecting more than one organ were characterized by:
- Presence of Spike protein and absence of nucleocapsid protein (SARS-CoV-2 only).
- Both arterial and venous systems had inflammation of the inner lining of the blood vessel wall.
- Larger vessels had evidence of inflammation in the elastic fibers of the aorta and larger vessels.
- Crystals consistent with cholesterol were identified in remote tissues and were thought to have been released from atheromata that were unroofed after the inner arterial lining were disrupted by Spike-caused erosion of the endothelium releasing debris and cholesterol emboli.
- Abnormal proteinaceous material consistent with amyloid was identified in multiple tissues.
- Unusual and aggressive cancer was identified and labelled “Turbo Cancer.”
- Atypical “clot” formation was identified.
- “True” foreign bodies from contaminated vaccines were identified.
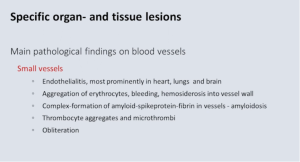
II. Specific Organ and Tissue Lesions involving the vascular system were characterized by:
Small Vessels:
- Heart, lung and brain had evidence of inflammation of the inner wall of blood vessels (endotheliitis).
- Evidence of bleeding (hemorrhage).
- Unusual blood clot formation comprised of amyloid, spike protein, and fibrin.
- Presence of small blood clots and clot forming blood cells.
- Obliteration of blood vessels.
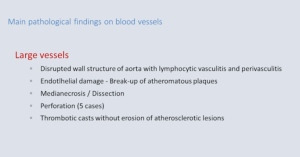
Large Vessels:
- Disrupted blood vessel wall of the aorta with associated lymphocytic vasculitis and perivasculitis.
- Damage to the inner lining of blood vessels with “unroofing” of cholesterol filled plaque.
- Disruption of the inner lining of blood vessels with dissection into the muscular middle layer of major arteries and subsequent dissection and aneurysm formation.
- Full thickness disruption of the aorta with exsanguination.
- Thrombotic casts.
III. Main Pathologic Findings (other organs) were characterized by:
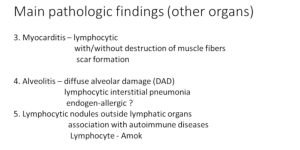
- Myocarditis – lymphocytic infiltration with/without destruction of muscle fibers / scar formation
- Alveolitis – diffuse alveolar damage (DAD) / lymphocytic interstitial pneumonia / endogen-allergic?
- Lymphocytic nodules outside lymphatic organs / association with autoimmune diseases / Lymphocyte – Amok
Dr. Burkhardt: “I have to tell you how it all started…

Soon after the first vaccinations were done in Germany, I was approached by relatives whose loved ones had died suddenly after the vaccination. They were autopsied, and the pathologist said, ‘Well, it’s all natural causes.’ The loved ones didn’t believe it. So, they went to other pathologists. They declined to look at these slides. And I was approached if I could give a second opinion.
And I said, ‘Well, of course I’ve done this in 40 years of pathology practice, and I will do it.’ After the first five cases, I realized that this was not an easy task and that it had to change from a second opinion to a scientific project. First of all, I was alone, then joined by Professor Dr. Lang of the University of Hannover. He’s also an experienced pathologist.
We started to look many times at these specimens that were sent to us, and which had come from the autopsies done by other pathologists. Now we are all in all 10 pathologists, coroners, biologists, chemists, and physicists that have joined to elucidate these cases.
I have to remind you that this is an ongoing examination. In the tables that will follow, I have different collectives because I cannot update every time I give a lecture.
In August 22 we had:
- 51 deceased and four living persons that we examined. (As of January 2023, we have 100 autopsies and 20 biopsies.)
- Of the 51 deceased, we had 26 men and 25 women.
- Age range: 21 to 94.
- Death occurred seven days to six months after the recent injection.
The vaccines are the ones that are usually in Germany. The task was to see if the vaccination had anything to do with the death occurrence.
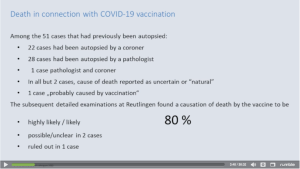
Among 51 cases:
- 22 cases were autopsies by coroners and usually without histology.
- 20 cases were autopsies by pathologists.
- One case by a pathologist and a coroner.
- In all but two cases the cause of death was reported as “Uncertain” and mostly as “Natural.” Whatever natural death is.
- It was stated the death could be possibly related to vaccination in only in one case.
After looking at all these specimens, histological slides in the microscope, we came to the conclusion that in 80% the vaccination had some influence on the death occurrence.
Death, of course, is a complicated occurrence, especially in an older person. But it may be influenced by vaccination, and there is usually a timely correlation. There’s one other study at Heidelberg University. They said in 30% that death after vaccination is correlated to the vaccination. (Schwab, et al.)
(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9702955/)


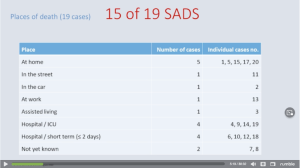
Most of the patients that we examined had a sudden death. They were found at home, on the street, or in the car. So, we don’t have changes caused by treatment like artificial respiration and so on. And of these, 15 of 19, were in the, in the category of what we call now sudden adult death syndrome (SADS). And you may notice this is a new term that has not existed before the vaccination.
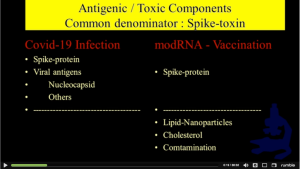
What did we do? First of all, we had to realize that there is a difference between the true Corona infection and the vaccination to the body. The Corona infection has protein and other viral antigens like nucleocapsid, while the vaccination only has a spike protein.
So, we have a common denominator. There is an overlap between the true infection and the vaccination; but, in the vaccination, we have other components that might be of relevance to pathological changes like the lipid nanoparticles, mRNA, cholesterol, and, in some cases, contamination, for example, by metals. The later has not been very closely examined until now.
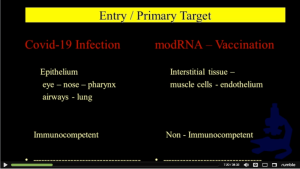
What is the difference between the entry and the primary target of the COVID-19 infection? The true infection goes to the epithelium: eyes, nose, pharynx, airways, and lung. This epithelium is immunocompetent. While, when we inject the vaccine, it goes into the interstitial tissue, into the muscle cells, the endothelium, and usually into the vessels. And these are not immunocompetent.
Now, what are the methods that we used? We used common histology, special stains, immunohistochemistry, and, in some cases, advanced physical chemical methods. From the beginning on, we were aware that this is a special challenge to us, because we don’t have a toxin that is coming from the outside, either by ingestion or by injection.
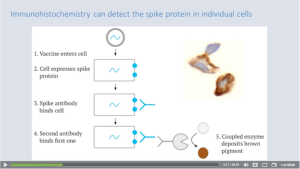
For example, systemic or histologic demonstration of toxins would not be of any significance; but we had to demonstrate a toxin that the body itself produced, and this was a Spike protein. And that’s why we very soon we developed a method to show the Spike protein in the tissues. (below)
And we differentiated this from the true infection by demonstrating the nucleocapsid antigen.
General Findings:
This is the first part of my presentation — general lesions expect affecting more than one organ.
Now, the first thing that we examined was the expression of Spike protein in the tissue. Then, we found that the endothelium is mostly affected, and there’s a disturbance of vessels generally, especially the larger vessels.
Then we have displaced unidentified vacuolar and crystalline particles, proteinaceous deposits, functional amyloidosis. We have unusual cancer manifestations, and we have clot formations in the blood and, in some cases, true foreign bodies. So, I will show you examples of these.
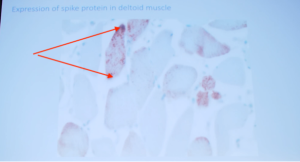
First of all, you’ve seen this already in the morning. This shows that we could confirm that the Spike protein is produced in the deltoid muscles where the vaccine is injected, but we could show it (Spike protein) in almost all organs, more or less explicitly.
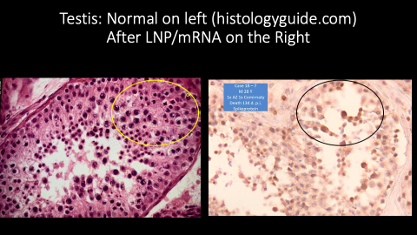
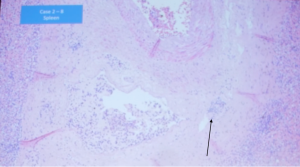
And here (Below) you see a case where we show the testis. You can see that, in this 28-year-old man who had a healthy son and who died 140 days after injection, the Spike protein is strongly expressed in the testis.
Normal (https://histologyguide.com/) on the left. Compare the circled region in a normal subject with the corresponding section in the 28-year-old man. Look at the lack of cells, not the color, as the stains are different.
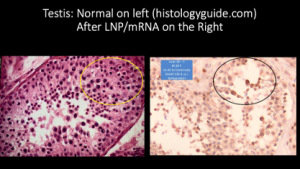
And you can see there are almost no spermatocytes (above right) in here, but there is strong expression of Spike protein in the spermatogonia.
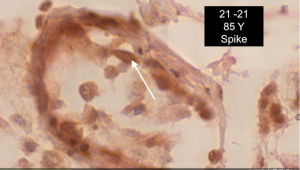
This is an old man. And you can see here, also, a strong expression of Spike in the spermatogonia. There’s not one single spermatozoa in this.
So, if I may make a personal comment, this is not a scientific comment. If I were a woman in fertile age, I would not plan a motherhood from a person, from a man, who has been vaccinated. I think these pictures are very disturbing for me.
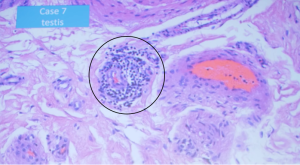
Lymphocyte Amok involving the testis.
In the testis, you can see this phenomenon which we called Lymphocyte Amok. We can see a lymphocytic infiltration and inflammation in the testes (above).
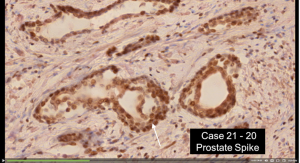
In the prostate gland, you can see a strong expression of Spike protein in this man.
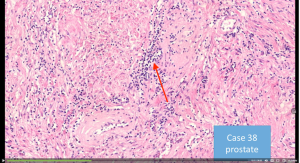
This is very disturbing, but its meaning we don’t know yet. This is inflammation in the prostate.
This is not a prostatitis. It’s a lymphocytic infiltration in the prostate.
But I come now to the main changes, the main damage that is done by the Spike protein which is induced by the vaccination.
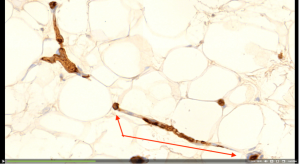
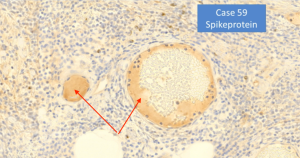
You can see here a Spike protein demonstration in a small capillary. You can see this is fat tissue. These are vascular structures, and you can see the Spike protein clearly and very distinctly marks capillary.
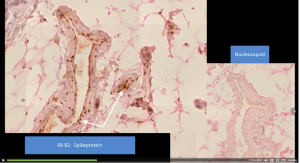
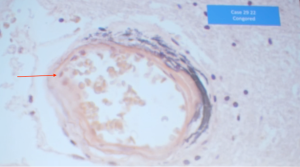
You can see here, on the left side, the spike protein in a small arteriole. The right inset box shows tissue with NO nucleocapsid protein thus no evidence of Covid-19 Spike. Only Spike from drug therapy is present.
Strong and distinct expression of Spike in the vascular endothelium of a small arteriole (below).
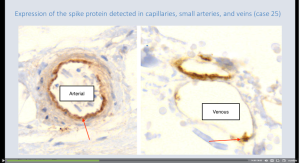
Inner part of these vessels has strong production of Spike protein that elicits a strong immunological reaction with destruction of endothelium. (Autoimmunity). Destruction of endothelium may be a major factor of the adverse effects of this vaccination.
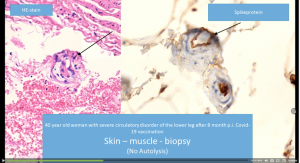
Swelling of the endothelium associated with impaired perfusion (circulation) in a lower leg eight months following vaccination. Endothelium clearly expresses Spike. Occluded vessel on the right.
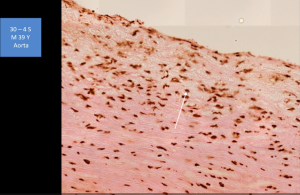
Aorta showing expression of Spike protein involving the endothelium (inner cell lining) and myofibroblastic (damaged heart muscle is replaced by fibrous tissue made by these cells) cells.

Foreign Body Reactions
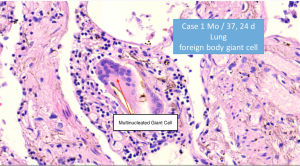
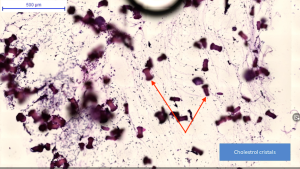
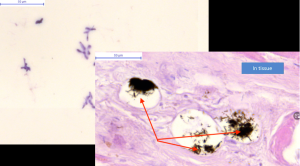
Giant cell formation with needle-like cholesterol crystals. (Giant cells are formed from fusion of other white cells such as macrophages in areas of chronic inflammation involving a variety of agents including foreign material such as surgical implants, bacterial, viral, parasitic or fungal infections. (Amy K. McNally, James M. Anderson, Macrophage fusion and multinucleated giant cells of inflammation, in Cell Fusion in Health and Disease, Springer 2011, pp 97 – 111 Dittmar and Zänker (eds.))
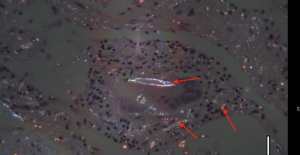
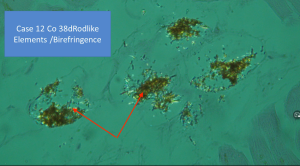
Birefringent (https://www.youtube.com/watch?v=WdrYRJfiUv0) microscopy shows small cholesterol crystals.
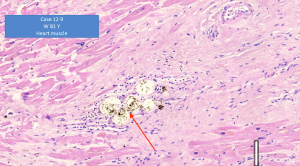
Heart muscle with rod-like structures in vaculoes made of cholesterol crystals.
Tablet-shaped larger objects with small, granular ones thought to be cholesterol crystals.
Left: Rod-like crystals in a cholesterol preparation. Right: Rod-like cholesterol crystals in heart muscle.
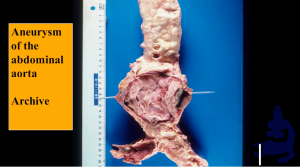
Archive photograph: Where does the cholesterol come from? Not from the injection, because the amount would not be sufficient. We now believe that the cholesterol comes from the wall of the aorta and atherosclerotic vessels. When the Spike attacks the endothelium, the cholesterol is released.
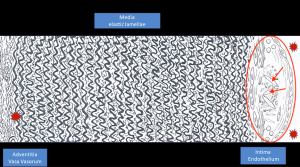
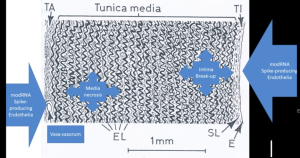
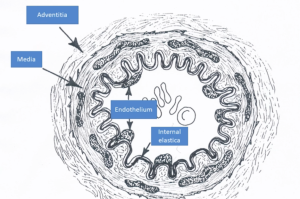
Schematic of arterial wall showing an atheromatous plaque, two red stars, containing spindle-like cholesterol needles on the right side, a thick muscular layer occupying about 80% of the full thickness of the vessel, and the external surface of the artery, the vasa vasorum. The vessels on the outside of the artery are also induced to form Spike proteins.
Atheromatous plaques could be set free into the body’s circulation, right side showing cholesterol and debris being released into circulation.

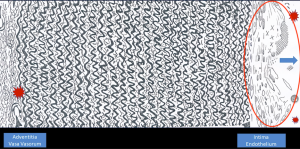
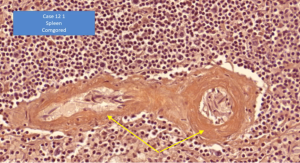
Vaccinated person with an atheroma laid open by the destruction of endothelium releasing the contents into the artery.
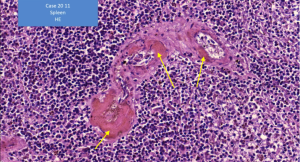
Same Case:
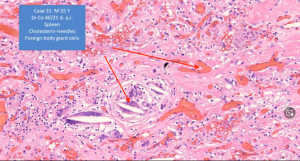
Cholesterol has come out of the atheromatous plaque of the aorta and lodged in a splenic vessel.
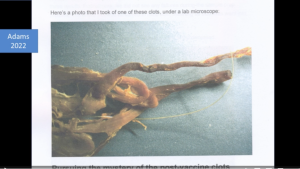
Strange clots have been associated with LNP/mRNA treatment.

Lady with damaged capillary endothelium with severe disturbance to the circulation. Sometimes she is unable to walk. Pictured here, on the sole of the foot, is red discoloration signifying inflammation in blood vessels called vasculitis.
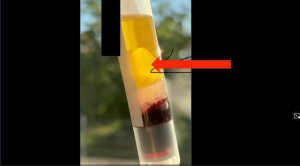
Blood was taken from this lady, and this clot formed in the serum after centrifugation and cooling in the refrigerator.
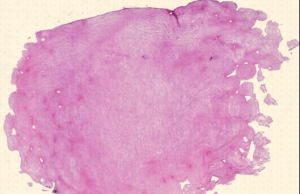
Clot stained and magnified. Proteinaceous practically acellular substance.

Examination of this clot was performed by specialized physical chemists, and they compared the contents of the plasma phase to the clot itself by mass spectroscopy. (Note: Proteomics is a branch of biotechnology concerned with applying the techniques of molecular biology, biochemistry, and genetics to analyzing the structure, function, and interactions of the proteins produced by the genes of a particular cell, tissue, or organism, with organizing the information in databases, and with applications of the data.)
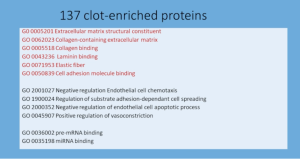
137 proteins were present in the clot and not in the serum. In Red are substances related to the endothelium, a sign of continuous damage.
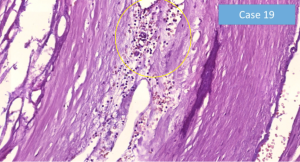
There are some hints that amyloid, a waxy translucent substance consisting primarily of protein that is deposited in some animal organs and tissues under abnormal conditions, could be formed of or by Spike proteins.
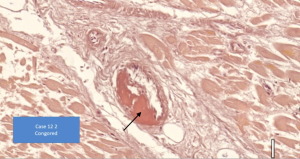
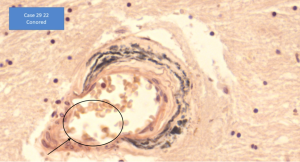
We very early found these deposits especially in vessel walls. You can see they are acellular (red stain) and compressed the vessel walls. Very early we had the suspicion this could be amyloid. (https://www.karger.com/Article/FullText/506696)
This could be proven by the special stain of Congo Red. (https://www.pathologyoutlines.com/topic/stainscongored.html)
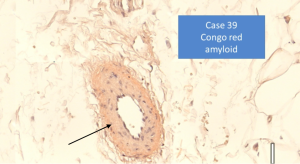
This is spleen and was found in the biopsy specimen of this lady that I showed you before (Case 39). So, she has some amyloid and, certainly, this has some meaning for the function of the vascular tissue. Also, we have these deposits in the brain.
Specific Organ and Tissue Lesions
We come to the specific on organ lesions. We have the small vessels showing destruction of the endothelium.
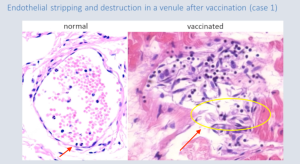
Here you can see the normal on the left side and the destructive capillary endothelium in heart muscle on the right side.
You can see that we can show Spike protein in these lesions.
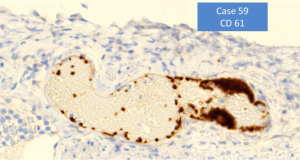
We can find a CD61+ thrombocyte apposition in these lesions. The CD (Cluster of Differentiation) designation refers to a convention of nomenclature for molecules of the cell surface of certain white cells. [https://www.hcdm.org/index.php/component/molecule/?Itemid=132] These white cell surface molecules are important to the function of the immune system. [https://www.immunopaedia.org.za/immunology/basics/cd-nomenclature/] Combined with CD41, the CD61 cell plays a role in platelet aggregation and clotting. [Principles of Immunophenotyping Faramarz Naeim, in Hematopathology, 2008, https://www.sciencedirect.com/science/article/pii/B9780123706072000028.]
This is the amyloid deposition in a small vessel in the heart muscle.
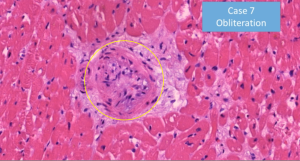
Occlusion (blockage or closing) of this vessel.
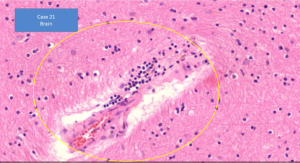
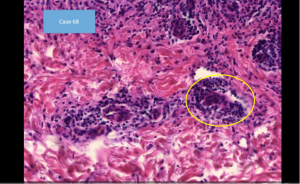
This is in the brain with inflammation of the small vessels.
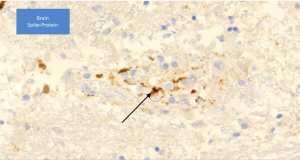
Here is Spike protein demonstration.
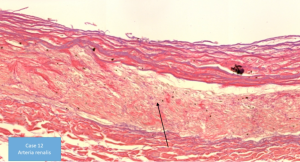
One very important finding, in our view, is the destruction and disruption of larger vessel walls.
We found media necrosis and breakup in these larger vessels.
Where do we find the media necrosis? We found it in idiopathic arteriosclerosis as shown here, and infection-toxic syphilis, Lathyrism and, apparently, Spike-induced.

This is an historic specimen from before World War I showing syphilitic destruction of the media (the middle, muscle layer of the artery).
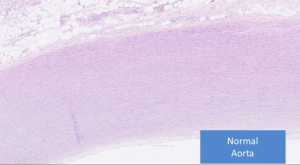
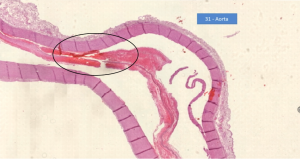
You can see what a normal aorta looks like this. It has a very regular, organized situation.
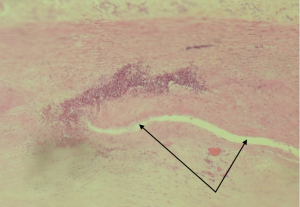
You can see here what we found in our deceased persons. You can see that the aorta is split.
The media (yellow) is necrotic, and there are inflammatory infiltrates, which in idiopathic form is not present. We can see that the media is largely destructed.
There are inflammatory infiltrates and destruction of the elastic lamella (layer of tissue) (yellow). You can see that the elastic lamellae are discontinuing. There are inflammatory infiltrates, which in the idiopathic form is not present.
We can see media (yellow) largely destroyed.
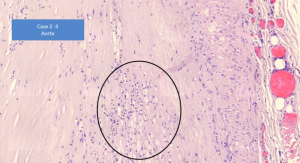
The inflammatory infiltrates
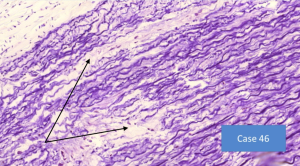
with destruction of the elastic lamella. You can see that the elastic lamellae are discontinuous.
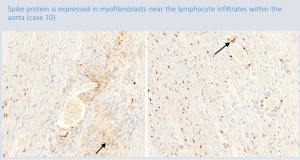
We can show here that the Spike protein expression in these hyperplastic myofibrils and also in the inflammatory infiltrate.

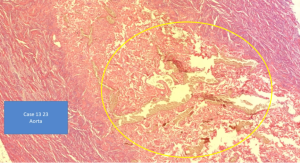
This is one of the autopsies that we did in a 56-year-old man.
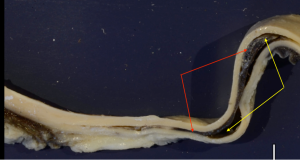
He had this, media[l] necrosis of the aorta. You can see here that the wall of the aorta is split (Red) into two parts, and in the middle there’s black blood. (Yellow)
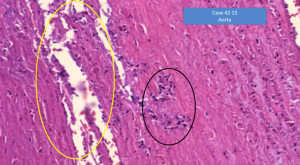
And this is a histological preparation. You can see very clear that there is medial necrosis,
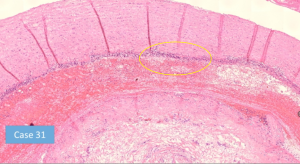
and you can see here that there’s a dense inflammatory infiltrate
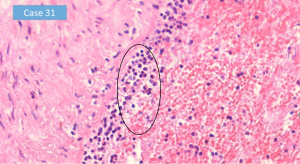
and a mass of histiocytes and macrophages.
First of all, we thought, we may be looking at a phantom; but, in Japan, they saw the same thing – aorta dissection, complicated by pericarditis and inflammation.
So, we did not only see this in the aorta, but also in the renal artery,
in the splenic artery,
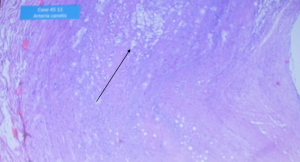
the carotid artery.
Here you can see vacuolar degeneration of the media.

Also seen in the vertebral artery.
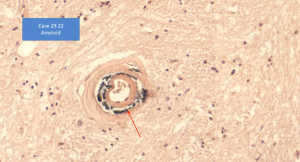
In the brain, there are residuals of bleeding. (Congo Red stain)
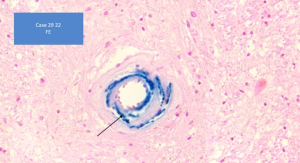
Blue stain represents Iron (Fe), so there has been bleeding in the small arteries in the brain.
You can see that the elastic lamellae are disrupted, and there are small, what we call aneurysms,
which might be ruptured at any time.
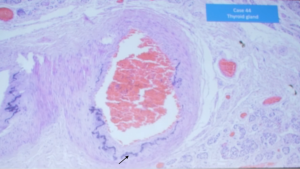
This occurred not only in the brain but also in the thyroid gland arteries. We saw these residuals of the destruction of the elastic lamella and iron deposition.

Here you can see the iron in the vessel wall.
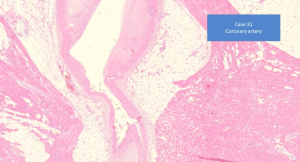
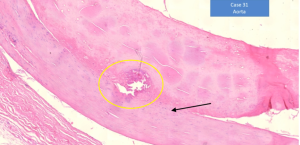
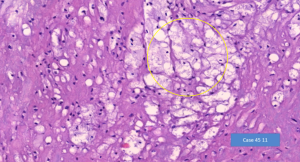
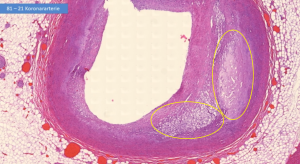
And now I come to the very delicate point because this might be the reason for some of the cases of a sudden death syndrome, because we see this in the coronary artery. At the bottom, you see a normal artery without arteriosclerosis. And you can see in the upper part, you can see there’s a cushion-like expansion and occlusion in the upper part. We saw this in many of the cases where the coronary artery was examined.
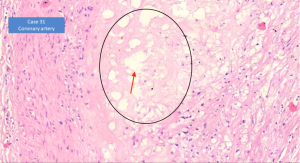
You can see here the medial necrosis with vacuolar degeneration (red arrow).
This is not arteriosclerosis. This is medial necrosis…
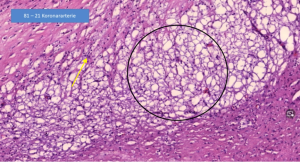
with some infiltration (yellow arrow) and vacuolar degeneration.
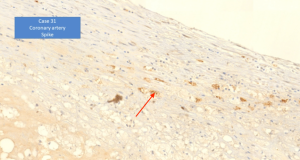
Here we demonstrate Spike protein in the inflammatory and myofibroblastic (https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.120.316958) cells.
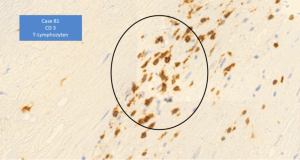
There are many T lymphocytes which, of course, cause immunological auto-aggression (autoimmunity).
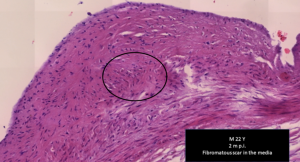
This is a case of a 22-year-old man who has a scar in the coronary artery. This is not an arteriosclerotic plaque.
I come to the meaning of these findings.
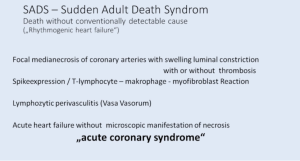
I think that the Sudden Adult Death Syndrome, means a death without conventionally detectable cause. Pathologists’ term this as ‘arrhythmogenic heart failure,’ which I don’t really know what they mean by that; but we have a focal medial necrosis of the coronary artery with swelling and luminal construction, with and without thrombosis.
We have Spike protein expression, T lymphocyte, macrophage and myofibroblastic reaction. We have lymphocytic perivascular inflammation, and this may be the underlying cause of what we call an acute coronary artery.
There’s no time that true necrosis of the muscle is manifest. So, there’s no pathologic findings of myonecrosis (dead heart muscle). We have no drugs outside the lymphatic organs showing an association of autoimmune disease.

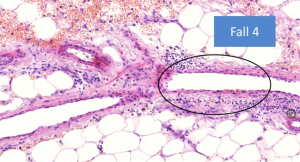
We are increasingly seeing younger persons with skin lesions. This is a 20-year-old man with vasculitis and atypical lichen of the skin. You can see here the vasculitis.
We have another case, a very impressive case of a 30-year-old woman two weeks after the second injection. She had zero general side effects but had massive skin lesions, rash, (inaudible), and bullae. She corresponded with me. She told me, ‘…my beautiful skin full of stains, my sexual life because I do not undress anymore.’
I left out some details. ‘I love the sea. It was taken from me because I cannot wear a bikini. Before I have felt fine. Now I get panic attacks without reasons.’

And these are the skin lesions that she never had before.
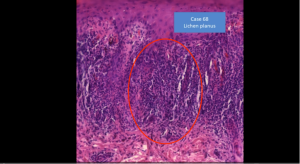
We see what we call, what is typical of an autoimmune disease, destruction of the basal cells with a band-like lymphocytic infiltration.
But in the lower part, you can see a small vessel, and this is atypical. It’s a vasculitis.
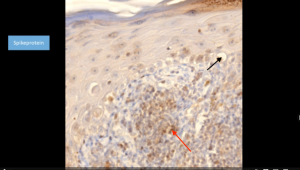
You can see the vacuolated basal cells are disrupted. And you can see again Spike (red arrow) protein can be demonstrated in the cell.
This is a vasculitis (yellow circle) and also in the small vessel are Spike protein.
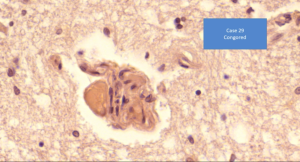
The last picture I will show you: the brain has Congo Red (stain) deposits which are very much like what we find in Alzheimer’s disease and…
Alzheimer’s disease is increasing.
There is an association of COVID-19, but as we see also with the vaccination.
Now, it’s unfortunately this was meant to be funny some years ago, but it has become a grim reality now. (Translation: I refer you to a Pathologist.)
I get about 20 to 35 telephone calls, because my name is now well-known in Germany and also in some adjourning country state, call me and they ask for help and they ask if I can do an examination and evaluation of their deceased relatives. All of themselves or the relatives with severe side effects.

I think I can close here. I could show you more cases. I have a collection, as I said, of 100 cases now, and it’s very hard to select what I want to show you. But I think I have been able to show you that there are very disturbing, very alarming findings that we have in the autopsy and also in the biopsy cases.
I think this is a reason to stop this vaccination at once.“
looks like good science to me
Mr M Smith had two shots of AstraZeneca
The last year and a half he has had to have his legs constantly dressed he has vascular problems repeatedly has ulcerated legs has now come up in psoriasis He has very bad balance causing him to fall on occasion , he can’t remember some things such as names and words , he gets horrific head aches that sometimes cause him to have nasal problems he sounds like he’s been in a boxing accident .
I have repeatedly told his doctors of these issues ( no outcome ) it is disgusting this man is 55 yrs old and now is like an 80 yr old he can hardly walk .
Why is no one commenting? The drug companies are completely silent as is the FDA, CDC, HHS, etc. Their silence is deafening and they have to know.
Can we all move this URL https://dailyclout.io/report-58-part-2-autopsies-reveal-medical-atrocities-of-genetic-therapies-being-used-against-a-respiratory-virus/ all over the planet? Everyong needs to see it ASAP!
Knew from the beginning these injections were bad news. No medical training, but we’ve to have our own cells produce spikes? Didn’t sound right so I refused thank god. Humanity is in big trouble.