

Report 56: Histopathology Series Part 1 – Autopsies Reveal Medical Atrocities of Genetic Therapies Being Used Against a Respiratory Virus
Summary:
Dr. Arne Burkhardt is one of eight international pathologists, physicians and scientists who were asked to perform a second autopsy, requested by friends and family of the deceased who were not satisfied with the results of the first autopsy.
Thirty autopsies and three biopsies were evaluated; 15 cases with routine histopathology (Step 1), three with advanced methods (Step 2), and some of the remaining 15 are included as illustrative cases.
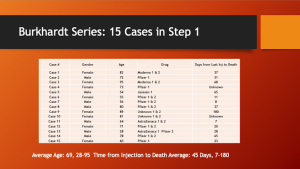
The Step 1 group included eight women and seven men aged 28-95 (average 69).
Death occurred seven days to 180 days following the first or the second Spike-Mediated Gene Therapy (SMGT) with COMIRNATY in eight, Moderna in two, AstraZeneca in two, Janssen in one and Unknown in two.
Place of death was known in 17 cases:
- Nine Non-hospital: five at home, one on the street, one in a car, one at work, one in an elder care facility
- Eight Hospital: four ICU, four died having been in hospital less than two days
Special stains were used to identify Spike and Nucleocapsid Proteins, with the following differential:
- COVID-19 (C-19) = + Spike + Nucleocapsid.
- SMGT = + Spike – Nucleocapsid.
Causation by SMGT: Very probable in five cases, probable in seven, unclear in two and no connection in one.
Lesions were on multiple organs including: Brain, Heart, Kidney, Liver, Lungs, Lymph Node, Salivary Gland, Skin, Spleen, Testis, Thyroid and Vascular.
Lymphocyte Infiltration, present in 14 of 20 cases (70%), was a common feature and involved multiple organs. Case 19 had at least five different organs involved. CD3+ Lymphocytes were dominant.
The Vascular System was targeted by Lymphocyte Infiltration in seven (35%) of the cases and included sloughing endothelium, destruction of the vessel wall, hemorrhage and thrombosis.
A condition called Lymphocyte Amok was described by Dr. Burkhardt: Lymphocyte accumulation in non-lymphatic organs and tissues that might develop into lymphoma.
Five cases of unknown foreign material in blood vessels were identified. The favored explanation for origin of this material was aggregated Lipid Nanoparticles (LNPs).
Multiple pathologic processes were involved: Apoptosis, Coagulopathy, Clotting/Infarction, Infiltration/Mass Formation, Inflammation, Lysis, Necrosis and Neoplasia.
Röltgen, et al. https://www.cell.com/cell/fulltext/S0092-8674(22)00076-9 found that COVID-19 depleted Lymphatic Germinal Centers (LGCs) whereas SMGT stimulated them, suggesting a possible origin of “Hunter/Killer” CD3+ Lymphocytes that are attracted to certain tissues, particularly the vascular system.
An expanded program of autopsy following SMGT is recommended in order to further understand the actions of SMGTs and to help formulate new treatments for the constellation of pathology associated with such drugs.
Burkhardt Group Conclusions:
- Histopathologic analyses show clear evidence of vaccine-induced autoimmune-like pathology in multiple organs.
- That myriad adverse events deriving from such auto-attack processes must be expected to very frequently occur in all individuals, particularly following booster injections.
- Beyond any doubt, injection of gene-based COVID-19 vaccines place lives under threat of illness and death.
- We note that both mRNA and vector-based vaccines are represented among these cases, as are all four major manufacturers.
Histopathology
This report is the first in a series in which harms from the Lipid Nanoparticle (LNP) Messenger Ribonucleic Acid (mRNA) therapeutics and other Spike-mediated products will be examined from the point of view of the pathologist, a medical doctor that studies specimens obtained from removal of tissue from living persons, bulk resection or biopsy, or after death. Such examinations make or confirm a diagnosis and provide a basis to determine causation of tissue mass or cause of death. Histopathology refers to the study of abnormal tissues.
Tissues are examined using careful inspection of specimens with the naked eye followed by examination by light microscopy employing a variety of different stains to highlight important features of cells, tissues and organs. A common stain used is hematoxylin and eosin, H & E for short, which stains nuclei blue, cytoplasm pink or red, collagen fibers pink and muscles red.
Many of the photomicrographs in this and subsequent articles will have been stained with H & E. Pathologists display sections prepared with H & E along with the magnification used, such as 40 times (40X) or 100 times (100X) magnification.
Immunohistochemical Stains for COVID-19 and Spike-Mediated Therapy
Special stains are vital to the identification of certain histopathology, such as cases involving Spike-mediated therapeutics. These examinations require special stains as outlined by Dr. Arne Burkhardt whose specimens and lecture notes will be the subject of this first report in a series.
Dr. Burkhardt discusses below the immunohistochemistry staining techniques necessary to differentially diagnose cell/tissue damage/organ from COVID-19, SARS-CoV-2 or something else, as well as specific cell types of interest such a T-lymphocytes and monocytes:
Immunohistochemistry to detect vaccine-induced spike protein expression.
Prof. Dr. A. Burkhardt
- Use anti-SARS-COV-2 spike protein/S1 antibodies to test for presence of spike protein in tissue samples. Always include myocardium and spleen tissue samples.
- If spike protein is detected, use anti-nucleocapsid antibody to examine expression of SARS-COV-2 nucleocapsid: presence of nucleocapsid indicates viral “breakthrough” infection, absence of nucleocapsid supports vaccine-induced spike protein expression.
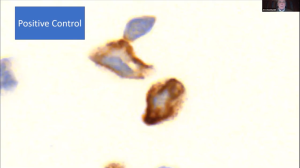
- Perform positive and negative controls using vaccine-transfected and non-transfected cell cultures.
Differential Staining to identify CD3 and CD68 cells and to Differentiate COVID-19 from Spike-Inducing Drugs
COVID-19 = Spike stain + Nucleocapsid stain +
LNP/mRNA = Spike stain + Nucleocapsid stain -:

- Spike, red arrow. b. Nucleocapsid, red arrow.

Without these special stains and without an exhaustive search of the specimens, no autopsy should be considered complete.
The internet is an excellent source for examples of both normal and pathological cells, tissues and organs.
A useful guide to have available when looking at the photomicrographs to follow is the Histology Guide at: https://histologyguide.com/.
This internet tool can be used to examine normal histology and compare it to the histopathology seen in Dr. Burkhardt’s slide deck which has been integrated with the transcription from his lecture on February 5, 2022.
Autopsy-Histology-Study on Vaccination-Associated Complications and Deaths
(Dr. Burkhardt’s slide deck was reproduced here and was integrated with the text derived from notes compiled from the voice recognition transcript with limited editing for readability with no intention to make substantive changes.)
Understanding Vaccine Causation Conference – February 5, 2022
World Council for Health
Dr. Arne Burkhardt
Pathologist
Reutlingen, Germany
“Dr. Arne Burkhardt, born in 1944 in Germany, a pathologist with more than 40 years diagnostic and teaching experience at the Universities of Hamburg, Bern, and Tübingen. He is the author of more than 150 original publications in international journals, currently engaged in autopsy studies of persons dying after taking the Covid vaccine.” Shabhan Palesa Mohamed

https://worldcouncilforhealth.org/multimedia/uvc-arne-burkhardt/
Dr. Burkhardt: I think it’s very, very, important to have an international communication on this subject, because last year in May, April, I was confronted with some relatives of persons who died after vaccination. And I tried to establish a national registry of these persons dying.
And I tried to get autopsies done in these persons, but the national associations of pathology here didn’t reply to this request by myself. So, when relatives continued to ask me, “Where can I get some solution to this problem?” finally, I said, “I can examine these organ probes that have been taken during autopsy, and we can try to get some other pathologists sent.”
These are the most relevant data on our study. We have eight cooperating pathologists, physicians, biologists; and they are internationally from Germany and other European countries, and also some outside of Europe.
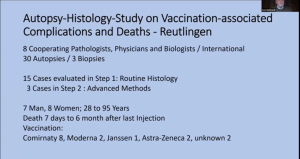
So, by now we have 30 autopsies and three biopsies from vaccinated persons. Fifteen cases have been evaluated in the step one that has reached Routine Histology. Three cases are in step two, Advanced Methods. I will explain what I mean by this.
And, just to give you a rough Impression, it’s seven men, eight women, 28 years to 95 years, death seven days to six months after the last injection and vaccination, the typical vaccinations that are used in Germany.
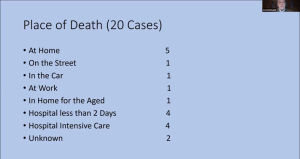
So, one important fact is that most of these persons that we examined have not died in the hospital, but at home, on the street, in the car. And that is very important, because, in these cases, we can exclude that there is interference with therapeutical measures like artificial respiration and things like that. So, only four were in intensive care medicine before they died.
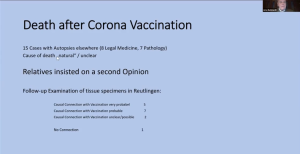
We had 15 cases with autopsy elsewhere which we examined in step one. And all of these 15 cases were classified by the pathologist of legal medical persons who made the autopsy as natural and unclear. And the relatives insisted on a second opinion. And we, in Reutlingen, in our group, looked at the specimens of the organs that were taken.
Our follow-up gave very probable correlation with the vaccination in five cases, probable in seven, unclear/possible in two, and no connections with only minimal changes we saw in one case.
So, what were the organs where we saw lesions? The target organs and the main lesions in her (sic) space, vascular lesions. Not only to the small vessels, the endothelium, but also to large vessel walls, to the muscular and elastic wall components.
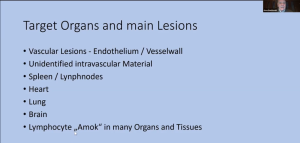
- In five cases, we found unidentified, intervascular material that might stem from the vaccination material. Then
- Spleen and
- Lymph nodes had changes.
- Heart,
- Lung
- Brain, and, finally, a phenomenon that we call
- Lymphocyte Amok. That means that we’ve found applications and nodular infiltration of lymphatic tissues and organs and tissues that are non-lymphatic.
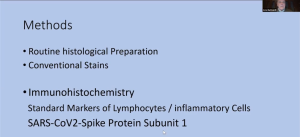
So, what are our methods?
- First of all, routine histological preparation with conventional stain, and then
- Immunohistochemistry first standard markers for lymphocytes/inflammatory cells.
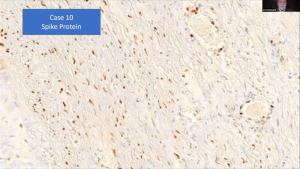
- But mostly this is one of the aims of this study, too, we try to demonstrate the Spike protein in the organs and tissues that were damaged.
And first of all, of course, we examine the specificity of our antibody to a Spike protein, and here a larger magnification. So, it seems to have a very high specificity for this Spike protein. And we did this in cell cultures
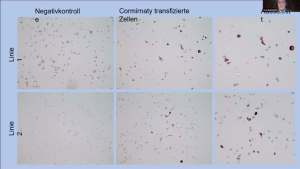
and you can see here net negative control, positive control.
And I will just show you a few examples of the tissue damage that I have listed before.
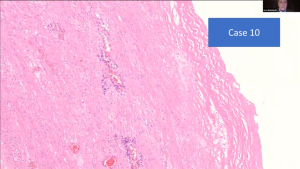
Blood Vessels, Endovasculitis, Perivasculitis and Vasculitis
So here (left) you can see a normal, small vessel, and you can see the endothelium that is like a wallpaper and very small, elongated spindle cell nuclei.
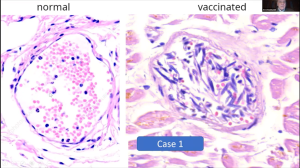
And here (right) in one of the cases, you can see that the
- Endothelium is in the lumen. And it is in there mixed with
- Lymphocytes and erythrocytes and the
- Nuclei are swollen.
So, in some cases, the small vessels even are completely destroyed by inflammatory infiltrates, mostly lymphocytes. And this proves to me that it is an intravital reaction and not an autolytic phenomenon caused by degradation after death.

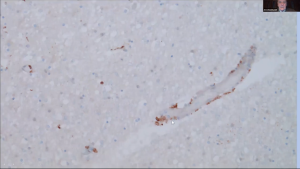
So, we get the Spike protein, immunohistochemistry on these cases, and we see, you see here a very marked and specific the mark of the endothelium in these patients. Rust-color stain more extensive in the smaller vessel wall.
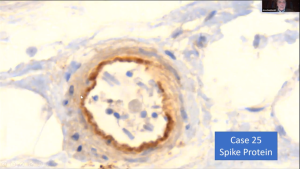
And not only in the small vessels, but also in the smaller arteries, you can see it in the inner part of the vessel. And you can see here there’s decimated endothelial cells.
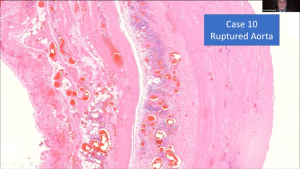
So, not as I said, not only the smaller vessels were affected, but also the aorta and the larger arteries and two cases have died of a ruptured artery. And, actually, we found arteriosclerotic changes; but, as you see here, it’s not very pronounced. But you can see inflammatory changes around in the deep layers of this aorta, and also you can see some disturbance of structure of the smooth muscle and the elastic fibers.
And if you have a higher magnification, you can see these small areas where the elastic fibers and smooth muscles are destroyed. And again, lymphocytic infiltration proving that it was an intravital process.
And here another case. We found it in, in five cases, so this cannot be a coincidence.
And we did the Spike protein stain, and you find a marked positive expermeation (expression) of Spike protein in the myofibroblasts of the arterial wall. This is the aorta.
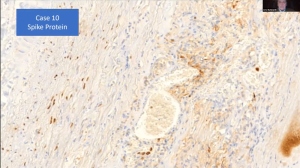
And also, in the vasa vasorum, you can see very strong expression of Spike protein in these areas. And this, I think, is a very important finding.
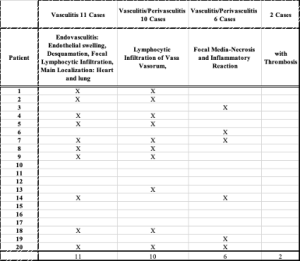
So how often did we see this vasculitis, this endovasculitis or some call it
- Endotheliitis, in 11 cases with focal lymphocytic infiltration, then
- Vasculitis perivasculitis in 10 cases,
- Focal media-necrosis in six cases, and
- Thrombosis caused on this area in two cases.
Spleen and Liver
So similar lesions are caused by toxins and drugs, cytostatic drugs, and in some food poisoning like lathyrism. And so, we think also here a toxic element, the Spike protein might be the causative agent.
Now another, other lesions that we saw in the spleen.
We first overlooked; but the more we looked, the more we found it. And this is one phenomenon that is known as onion skin arteritis of the spleen, which is seen in some autoimmune diseases like lupus erythematosus. And, in the course of these arteriolitis, we saw focal destruction of follicular arteries in the spleen and products of the lymphatic follicles.
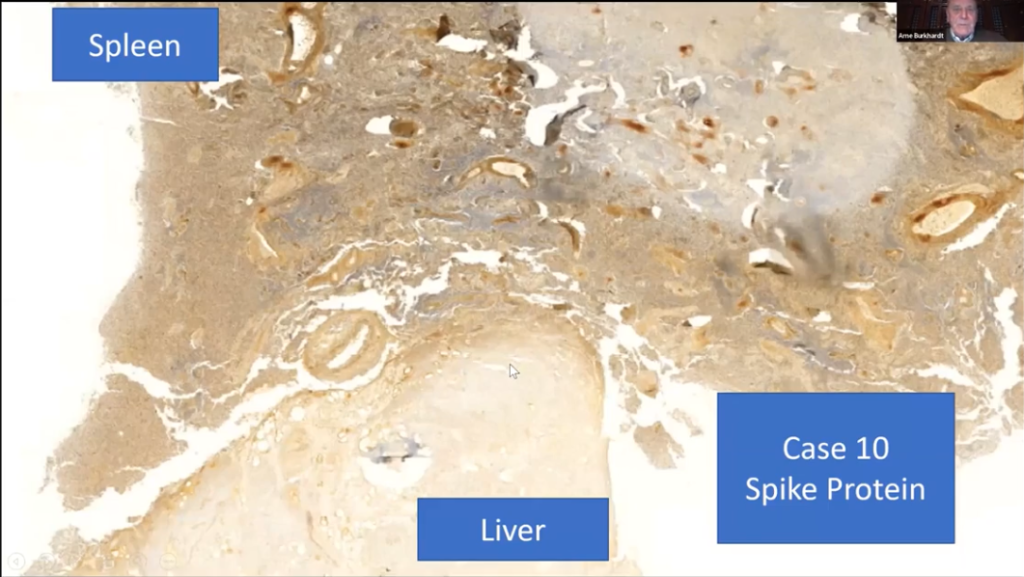
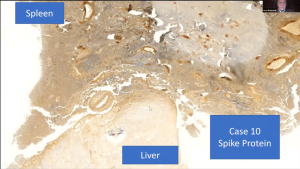
Now, first of all, this picture is an overview of two organs in one paraffin dock. You can see here the liver and here the spleen. And so, both organs have had the same preparation, the same fixation and everything.
So, you can see easily that the liver is practically non-reactive. You can see some small vessels in the endothelium are positive, but the liver itself is negative.
And then, in contradiction, the spleen has a very pronounced mark around the vessels and small arterioles.
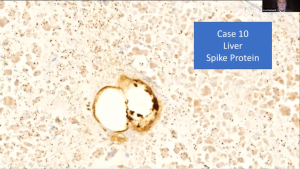
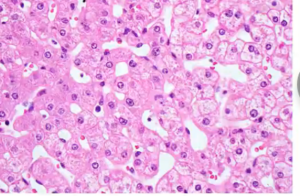
This is a liver now; and you can see the liver cells itself are negative, but the small vessels, the capillaries, have a strong, positive reaction of the endothelium (indicative of Spike protein).
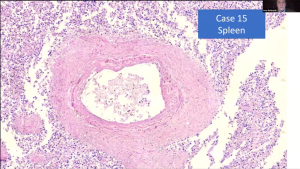
Spleen showing the “onion skin” phenomena that is seen in some autoimmune diseases. Concentric layering is seen in the thickened arterial wall. Surrounding the artery, hypercellularity is visible with intense nuclear material reaction (blue dots).
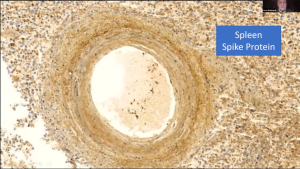
And this is this reaction that is called the onion skin phenomenon, which is seen in some autoimmune diseases. You can see the wall of the artery is split up in, in a way. And also, here we can show, as we saw on the overview that there’s a strong reaction for the Spike protein.
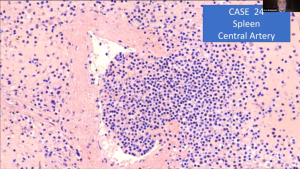
And this is a phenomenon that none of the pathologists that I work together have ever seen. This is a small follicular artery in the spleen; and you can see the wall has a focal defect, and the lymphatic tissue is protruding into the vessel.
Lymph Nodes, Pseudolymphoma, Neoplasia
So, it also changes in the lymph nodes. Densely packed with, possibly, atypical lymphocytes that are locally invasive suggestive of neoplasia?
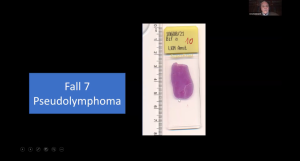
We have seen a case of a pseudolymphoma, as I can show you here. It’s at least three centimeters large.
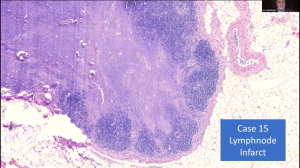
And then, in another case, we saw a focal central infarct of the lymph nodes. Infarction is suggestive of neoplasia, as cellular proliferation is so aggressive that it outstrips the local blood flow leading to infarction.
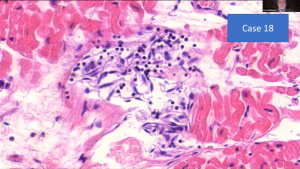
Heart
Now the myocarditis is now, I think, it’s internationally known that it is a side effect of vaccination.

And you can see that, in our cases, we saw these lymphocytes marching up in the small vessels here. You can see the intact muscular fibers.
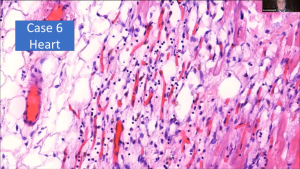
And, in this case, you can see that they (cardiac muscle fibers) are destroyed by the lymphocytes that are infiltrating in contradiction to true infarct of the cardiac muscles. Do not see granulocytes (granulocytes are white blood cells also known as polymorphonuclear leukocytes that predominate in cases of non-vaccine-related myocardial infarction) in these areas. Only very few when some macrophages, of course.
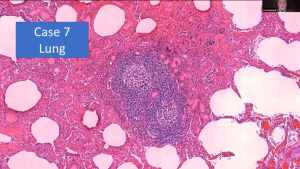
Lung
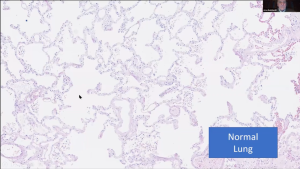
So, we come to the lung here. You see a normal lung. You can see here all the white areas of the lung alveoli.
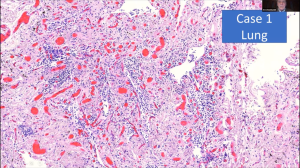
And what we found are very pronounced changes in which you might call a lymphocytic alveolitis, lymphocytic interstitial pneumonia. And you can see that only very few areas where there are still alveoli.
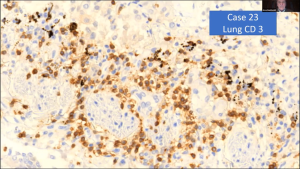
The infiltration is mostly T lymphocytes, CD3+. (T Helper? T Cytotoxic? or new Species: T Neoplastic Lymphocyte?) Note the high concentration of Spike protein represented by rust-color stain.
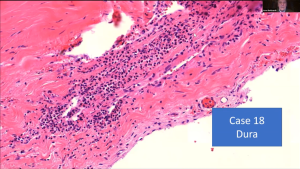
Brain
Very important are the changes that we found in the brain.
We found a transfection-associated encephalitis, then lymphocytic infiltration, and focal destruction of intracerebral and arachnoidal blood vessels, subarachnoidal hemorrhage, without an aneurysm, in young people, focal lymphocytic infiltration is also in the Dura mater. In one case, partial necrosis of the hypophysis (pituitary gland).
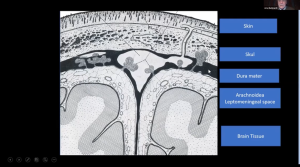
Now this, just for those that are not familiar, this is Dura mater. And here we found infiltration by lymphocytes. This is the arachnoidea where we found perivascular inflammation, and we also found it in the brain. This is Dura mater; you can see this focal infiltration by lymphocytes.
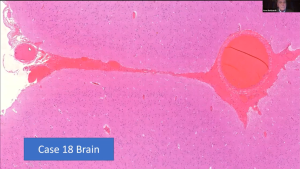
This young 26-year-old died of hemorrhage (arrow at 9 o’clock). No aneurysm.
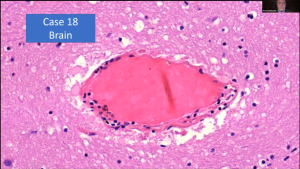
You can see that the vessels in the brain and in the [inaudible] have a focal lymphocytic infiltration, and probably that caused a rupture. Also,
infiltration by lymphocytes.
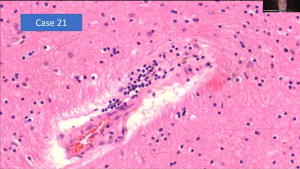
And this is a case of encephalitis which we observed.
And in this case, we could demonstrate a Spike protein, again, in the smaller vessels. And here, a small artery; here, very pronounced, positive reaction.
Another area where you can see this definitely and very clear positive cells. It’s mostly in the small vessels, but also in some neural cells.
Lymphocyte “Bee-Hiving”
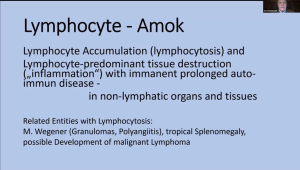
And now in a phenomenon that we call the Lymphocyte – Amok, which is a lymphocyte accumulation and lymphocyte predominant tissue destruction outside of the myocardium and the lung where I’ve already demonstrated this.
It’s definitely the danger of a prolonged autoimmune disease. And this we found in non-lymphatic organs and tissues. There are some autoimmune diseases which are related to this phenomenon.
And this is in the lung. In the lung, sometimes you find small lymphocytic elements; but I have never seen before a quasi-lymph node with reaction centers and activation.
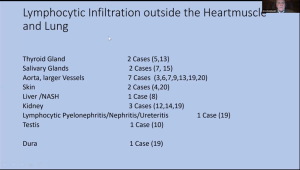
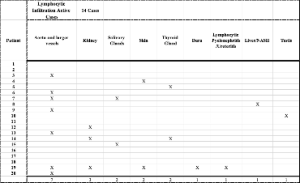
And this is the frequency that we found of these lymphocytic infiltrations, the thyroid glands, the salivary glands. And by the way, of course, we found this in two cases, but we only had these organ specimens in two cases. So, it was found in 100% of the cases that we examined.
So, in the aorta, I showed you before, skin liver, kidney, lymphocytic pyelonephritis, nephritis, in the testis, in one case, and in the Dura, I showed you this phenomenon.
Fourteen cases with lymphocytic infiltration outside of the lungs:
- Seven cases with aorta and large vessels;
- Three cases with kidney;
- Two cases each with salivary glands, skin, and thyroid;
- One case each with Dura, pyelonephritic/ureteritis, liver/NASH, testis;
One patient (#19) had five sites of lymphocytic infiltration: aorta/vessels, kidney, skin, Dura, lymphocytic pyelonephritis/Ureteritis
So, these are the organ changes.
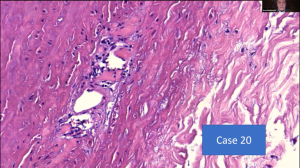
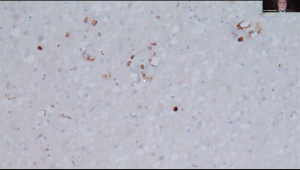
Unidentified Foreign Material in Vessels
And, just as the last lesions that I would like to show you, is unidentified foreign material in the vessels, especially in the spleen vessels.
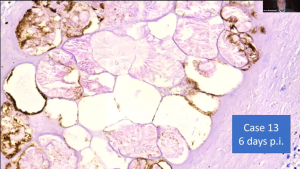
And this is something that we could not identify. (White arrow at 9 o’clock.)
No pathologists that have looked at it know what it is.
First, we saw these cells, but they have an inner structure like [inaudible]; and then we thought it might have been a contrast material, but this patient died at home and was not in the hospital for a long time.
And this was one case in the spleen, and this is another after some longer period of time.
So, our theory is that these are the nanolipid particles, which when they come into the body and are warmed up, which coalesce and form larger particles that might, at one point, stick in the system, in the vessel system. And this was one case in the spleen,
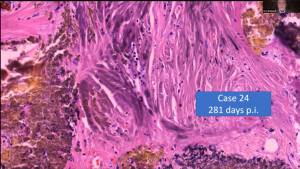
and this is another. The last one was only a few days, and this is after some longer period of time. I might add that this is a coincidental finding because this was not macroscopically seen, but we had it by coincidence in our sections.
Case Report
I will show you a case report over natural death uncovered as caused by vaccination-induced vasculitis of the coronary artery.
It was a 54-year-old man, two vaccinations, and he died 123 days after the second vaccination.
And there was no doubt this was myocardial infarct. The primary autopsy was contested.
They saw a discoloration of the cardiac muscle and said, “Well, yes, he died of a myocardial infarct;” but then we did histology of the coronary artery, and we found these changes.
And, in addition, in the muscle we found the myocarditis, as we found typically in the other cases, as I have shown.
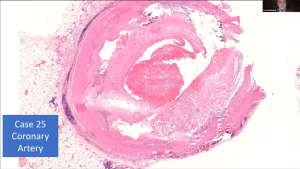
Now this is the coronary artery and, yes, you see it’s clearly there; there is thrombus formation inside. And yes, there are arteriosclerotic changes.

But look at these areas and here around the vessel. There’s definitely inflammatory reaction. (At 8 to 10 o’clock outside the pink thrombus in the coronary artery to the right of the clue staining tissue.)
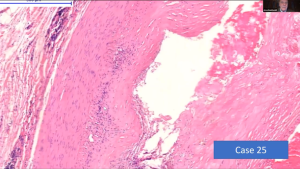
And you can see this disturbance of texture of the smooth muscle and the myofibroblasts here, and you can see also some discrete lymphocytic infiltration.
And then, around the vessel, there’s this dense lymphocytic infiltration.
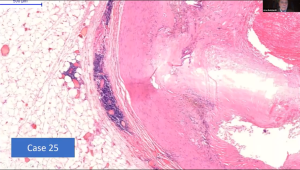
So, we concluded that the vessel, the coronary artery, had an inflammation induced by the vaccination, by the Spike protein.
And the thrombus was built on the ground of these inflammatory changes and led to the infarct, which definitely was present.
But also, the fact that there was a concomitant, myocarditis, very strong evidence that this secondary, because of the vaccination.
And we spent many, many hours looking at all these slides.
And for a long time, we were thinking, ”Well, we are chasing a phantom;” and we looked at each other and ask each other, “Do you see this? Do you see this? Is this real?”
And we are now at a point, and especially after we could prove the presence of Spike protein for months after vaccination, we are come to the conclusion, no, we are not chasing a phantom.
Further studies are necessary, and I think it’s a very exciting field that we are coming to, but also a very depressing and very scary phenomenon.
Thank you.
Dr. Mark Trozzi:
So, I’m going to pick two questions. One is very sweet, and it’s an anonymous attendee who says, “Professor Burkhart, do I understand that you came out of retirement to help us, the people of the world in need?”
“Well, actually, I was just retiring a few months before I started to study. I gave back my license for the health insurance in April last year. And, in May, I was contacted, and they asked me if I would do this study. And I, by the way, I also have some consulting contracts with some other laboratories.
So, I’m not retired in the way that I am not active anymore, but I’m retired in the sense that I am not responsible to anybody, and that I cannot be thrown out of my job. I’m independent.”
An underlying theme of the histopathology of LNP/mRNA harms is involvement of vascular structures, arteries and veins. Table 1 below identifies vascular involvement in the 20 cases.
Table 1: Histopathology from LNP/mRNA Involving the Vascular System
(Burkhardt Series)
Lymphocytes of various types have been identified in proximity of cellular, tissue and organ damage and may come from activated germinal centers as identified by the Boyd group at Stanford, https://doi.org/10.1016/j.cell.2022.01.018. [Röltgen, Katharina, et al. “Immune Imprinting, Breadth of Variant Recognition, and Germinal Center Response in Human SARS-COV-2 Infection and Vaccination.” Cell, Elsevier, 24 Jan. 2022, https://www.cell.com/cell/fulltext/S0092-8674(22)00076-9.]
Table 2: Possible Origin of “Activated” Lymphocytes
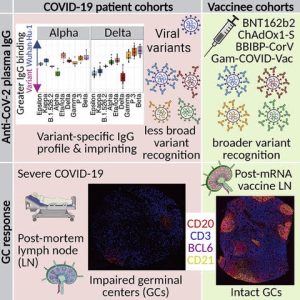
This study found that COVID-19 impairs the lymph node germinal centers but transfection with Spike-based therapeutics was found to stimulate the germinal centers:
“The biodistribution, quantity, and persistence of vaccine mRNA and spike antigen after vaccination and viral antigens after SARS-CoV-2 infection are incompletely understood but are likely to be major determinants of immune responses.”
Presumably this also means that the activated lymphocytes produced by the ongoing activity of the transfected mRNA have not been studied as well including potential detrimental effects such as autoimmunity from protein mimicry and neoplasia from genome dysregulation.
“The observed extended presence of vaccine mRNA and spike protein in vaccinee [lymph nodes (LNs)] [germinal centers (GCs)] for up to 2 months after vaccination was in contrast to rare foci of viral spike protein in COVID-19 patient LNs.”
This is an important difference between COVID-19 and the Spike-based therapeutic products and at least partially explains the long-time course of harms from the Spike-producing products that range from seven to 180 days in the Burkhardt series (average 45 days).
Table 3: Lymphocyte-Associated Organ System Pathology from Spike-Producing Therapeutics
Consider the action of mRNA on the Lymphatic Germinal Centers with activation of lymphocytes while, at the same time, Spike-related foreign proteins are being produced in distant tissues and organs.
Are these activated lymphocytes released from the Germinal Centers and then hunt down and attack organs and tissues producing Spike proteins that are recognized as foreign? Do these activated lymphocytes produce tumors?
Table 4: Organ System Harms from Spike-Producing Therapeutics
Burkhardt Series
| Organs |
| Brain |
| Heart |
| Kidney |
| Liver |
| Lungs |
| Lymph Node |
| Salivary Gland |
| Skin |
| Spleen |
| Testis |
| Thyroid |
| Vascular |
As cases accrue, the number of organs is expected to increase.
Table 5: Histopathology: Mechanisms of Injury
| Histology | Definition |
| Apoptosis | Cell Death |
| Coagulopathy | Clotting |
| Infarction | Sudden Loss of Blood Supply |
| Infiltration | Abnormal Accumulation |
| Inflammation | Complex Chemical and Cellular Cascade that clears debris, microbes and begins Repair |
| Lysis | Dissolution |
| Necrosis | Death |
| Neoplasia | Pre Cancer or Cancer |
Autopsy, Histopathology and Determination of Cause of Death
Case Report:
Hunter Brown, Age 21
![]()
[https://taskandpurpose.com/news/air-force-academy-cadet-dies/]


“A coroner has determined that Air Force Academy Cadet 3rd Class Hunter Brown died of a blood clot in his lungs that was caused by an injury to his left foot that he sustained during football practice weeks earlier, according to a copy of Brown’s autopsy report that was provided to Task & Purpose.
The final diagnosis also noted enlarged liver, heart and spleen for Brown, a Louisiana native who was 6-foot-3 and 292 pounds at the time of his death at the at the age of 21.” [https://gazette.com/sports/autopsy-for-air-force-football-player-hunter-brown-released/article_05da22d4-a242-11ed-88b1-b767cb0e502b.html]
Cadet Brown had a fracture dislocation of the base of his second toe that was repaired surgically. Blood clots (superficial or deep venous thrombosis) following surgery for an injury of this type are exceedingly rare and, when they occur, they seldom break free and travel to the lung (pulmonary embolus).
Selby, Rita MBBS, FRCPC, MSc*,†; Geerts, William H. MD*; Kreder, Hans J. MD, MSc‡; Crowther, Mark A. MD, MSc§; Kaus, Lisa*; Sealey, Faith RN*. A Double-Blind, Randomized Controlled Trial of the Prevention of Clinically Important Venous Thromboembolism After Isolated Lower Leg Fractures. Journal of Orthopaedic Trauma 29(5):p 224-230, May 2015. | DOI: 10.1097/BOT.000000000000025
The primary effectiveness outcome was clinically important venous thromboembolism (CIVTE), defined as the composite of symptomatic venous thromboembolism within 3 months after surgery and asymptomatic proximal deep vein thrombosis on DUS. The primary safety outcome was major bleeding.
Two hundred fifty-eight patients (97%) were included in the primary outcome analysis for effectiveness (130: dalteparin; 128: placebo). Incidence of CIVTE in the dalteparin and placebo groups was 1.5% and 2.3%, respectively (absolute risk reduction, 0.8%; 95% confidence interval, −2.0 to 3.0).
There were no fatal pulmonary emboli or major bleeding. [https://pubmed.ncbi.nlm.nih.gov/25900749/]
Assuming Hunter Brown had an extremely unlikely fatal pulmonary embolus, such an event is sudden and catastrophic with no time to develop associated pathology in the liver, heart and spleen.
Hunter Brown’s medical event and the associated autopsy findings do have an excellent match with the pattern of organ damage from Spike-producing therapeutic agents (SPTA). In a report of what the authors believe was the first autopsy in a Spike-producing therapeutic associated fatality, nine different organs or tissues were damaged by the LNP/mRNA.
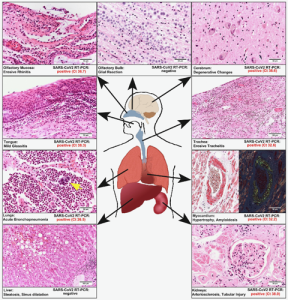
[https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8051011/pdf/main.pdf]
Conclusions from Drs. Bhakdi and Burkhardt:
- “Histopathologic analyses show clear evidence of vaccine-induced, autoimmune-like pathology in multiple organs.
- That myriad adverse events deriving from such auto-attack processes must be expected to very frequently occur in all [COVID-vaccinated] individuals, particularly following booster injections.
- Beyond any doubt, injection of gene-based COVID-19 vaccines place lives under threat of illness and death.
- We note that both mRNA and vector-based vaccines are represented among these cases, as are all four major manufacturers.”
(Bhakdi and Burkhardt, On COVID vaccines: why they cannot work, and irrefutable evidence of their causative role in deaths after vaccination. Transcript from Live Streamed presentations at the Doctors for COVID Ethics Symposium December 10, 2021. https://doctors4covidethics.org/on-covid-vaccines-why-they-cannot-work-and-irrefutable-evidence-of-their-causative-role-in-deaths-after-vaccination/)
Thank You!
Does the production of the spike protein continue indefinitely, or does it stop/slow down at some point?
This is the million dollar question. We have known for over fifty years that reverse transcription occurs with retrovirus (hence the name ) . Sars covid 2 is a retrovirus therefore the ability exists to go from RNA to DNA and back.
Some studies in Sweden have confirmed this occurring in human liver cells.. so the steady production of covid Mrna from the host DNA ia a problem for all of those injected with Mrna to produce the spike glycoprotein antigen. Further research is needed as a matter of urgency.
Just heard via Dr. Campbell that a Danish study has found that mRNA NLP’s are still in the blood 28 days after vaccination.
https://www.youtube.com/watch?v=fWVxVd6IGgg
Conny I think in this danish study the free Mrna was found in the blood and not the NLPs. This is significant as the discovery was found accidental in Hep C patients, and most likely as a result of destruction of the liver cellsby the HepC virus and release of the cell inclusions into the circulation, this includes the Mrna for the spike . This in my opinion cofirms the occurrence of reverse transcription of spike Mrna in the human liver cells. I will state again more research needed as a matter of extreme emergency
This is horrific! But is this vaccin same vaccine President Trump did the emergency production? How many have died from the first jabs 2 yrs ago? Or Did Biden regime “change the jab BOOSTER’S”(Joe’s watch) after he took power and now all these innocent Americans are dying? Did they( Pfizer/ccp?) Change the juice to kill? It seems more of our country men/women dying since JB took over..You’re saying a year or 6 months after ,since jb took over!!! All those booster made AFTER President Trump! I notice that some folks are ok after vaccine so is it not affecting everyone that way or its just not happening to them ,yet! My sister passed out at the airport after her booster 2 months ago shes almost 80 thank you for saving lives with this endepth analysis God protect you!
Last month a California teen on collapsed at home on her 17th birthday and required resuscitation. Subsequent exploratory surgery revealed an inexplicably ruptured spleen. She thankfully survived the trauma and is now at home recovering. This report’s section on spleen lesions made we wonder if there’s a relationship. Some of the details are at this link:
https://gofund.me/db28be29
This style of conscious ignorance and sincere stupidity are evident from sea to shining sea, America is being destroyed from every angle of attack, and is represented by any histologic examination; just a dying body at the hands of the demonic barbarians across all walks of life.
Hm. Out of the hundreds of millions of people vaccinated, the “experts” are basing their findings on 30 autopsies. I just heard an interview with Naomi Wolf. The AVERAGE age of the person autopsied was 69. I’m shocked, shocked that some of these people had health problems.
Questions for you: (1) by “experts” do you imply you are more qualified than these pathologists on the subject matter? (2) do you have any idea how much work it is to perform histology studies on multiple organs in ONE autopsy–let alone 30? (3) out of hundreds of millions of people who have been injected do you know how many died shortly after? Pfizer’s own records captured 1200+ deaths reported in the first 90 days after the start of global distribution. (4) how many more are injured than dead, 10x? 100x? (5) yes, dead and injured are a small percentage, but do you want to be among them? (6) yes, COVID presents serious risks to some, but why shouldn’t the risks of these shots also be thoroughly studied so that we each can make our own risk/benefit assessment and choose whether or not to take these shots?
dont fight it…. its real report. mrna is a death jab
Top pathologists have examined disputed cause of death cases. In the great majority of these cases, they found clear evidence that their c19 vaccination had killed them. Autoimmune attack in multiple organs. If vaccine injury is rate, you’d not expect to find it in a small sample. Yet they find vaccine characteristic injuries wherever they look. The implications are that the Great bulk of sudden unexplained deaths & the excess all causes mortality is due to c19 vaccines. Estimates vary, but between 500,000 & 1,000,000 people in USA are dead who would likely be still alive were it not for these injections.
69 is my age. A few months after double vax physically forced on me, my prostrate has swollen. I suppose it might be a co-incidence. I insisted on the aspiration method, that is not plunge into a vein, as advocated by Doctor John Campbell. He advocated the vaxes and took them himself. He says he now has high blood pressure. Might be a co-incidence.