

Report 70: Histopathology Series Part 4c – Autoimmunity: A Principal Pathological Mechanism of COVD-19 Gene Therapy Harm (CoVax Diseases) and a Central Flaw in the LNP/mRNA Platform
This report is Part 4c in a series. It follows Part 1, “Report 56: Autopsies Reveal Medical Atrocities of Genetic Therapies Being Used Against a Respiratory Virus;” Part 2, “Report 58: Part 2 – “Autopsies Reveal Medical Atrocities of Genetic Therapies Being Used Against a Respiratory Virus;” and Part 3, “Report 61: Part 3 –Ute Krüger, MD, Breast Cancer Specialist, Reveals Increase in Cancers and Occurrences of ‘Turbo Cancers’ Following Genetic Therapy ‘Vaccines’,” “Report 64: Part 4a – Re-Humanizing Data Using ‘Intramyocardial Inflammation after COVID-19 Vaccination: An Endomyocardial Biopsy-Proven Case Series;“ and “Part 4b – Rhabdomyolysis – a.k.a., “Jellied Muscle” – After mRNA Gene Therapy Injections.”
Introduction
A new class of illness, termed within this report as CoVax Disease, is now warranted. CoVax Disease encompasses multiple pathological mechanisms of which autoimmunity occupies a central position.
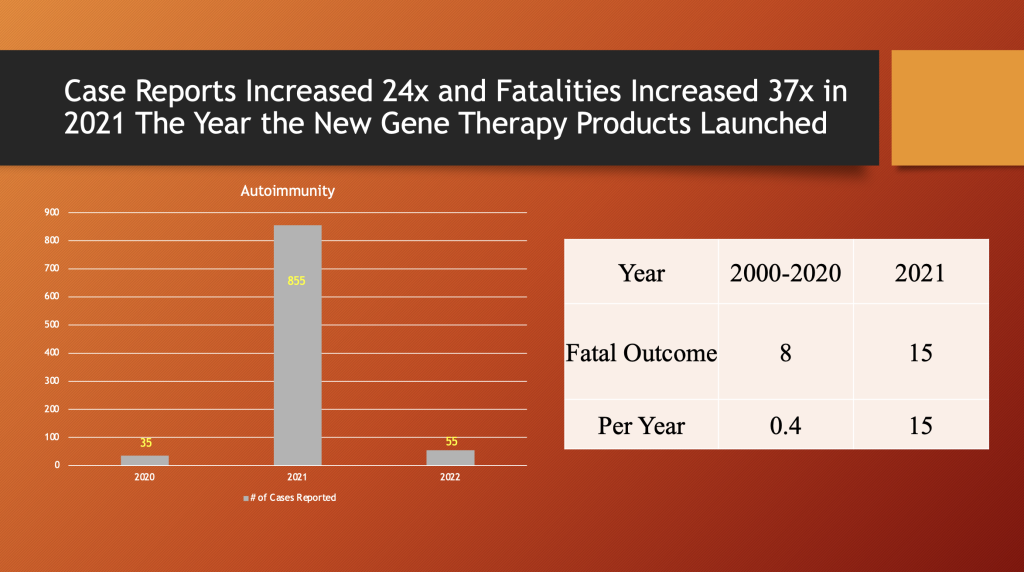
In this report, the reader will learn that autoimmunity cases reported to the Vaccine Adverse Events Reporting System in the U.S. increased 24 fold from 2020 to 2021, and annual autoimmunity-related fatalities increased 37x in the same time period.
mRNA “vaccines” are now associated with changeable disease manifestations that come from the widespread biodistribution of the mRNA gene therapy products that enter host cells and then translate mRNA code into Spike proteins that the host immune system does not recognize. Those unrecognized proteins prompt an immune response from the host that targets and destroys Spike proteins in host tissues and organs, sometimes dramatically and even fatally. mRNA “vaccines” have made the “vaccinated” human body its own worst enemy.
I: Autoimmunity: Definition, Prevalence and Clinical Variation
“Auto” is from ancient Greek word αὐτός meaning “self.” (https://www.perseus.tufts.edu/hopper/morph?l=au%29to%5C&la=greek&can=au%29to%5C0&prior=ou)k&d=Perseus:text:1999.01.0167:section=363a&i=1#lexicon.) When combined with immunity the term applies to medical conditions resulting from a destructive immune response to oneself. This response comes in the form of both antibody and cellular attack on one’s own tissues and varies from involvement of a single organ to multiple organs or widespread systemic manifestations. (https://pathology.jhu.edu/autoimmune/prevalence/)
Johns Hopkins Medical School Department of Pathology gives the prevalence of autoimmune illnesses in the United States as 10 million, or approximately three percent of the population behind obesity 115 million, cardiovascular disease 66 million, Type 2 diabetes 50 million and all cancers 13 million. (https://pathology.jhu.edu/autoimmune/prevalence)
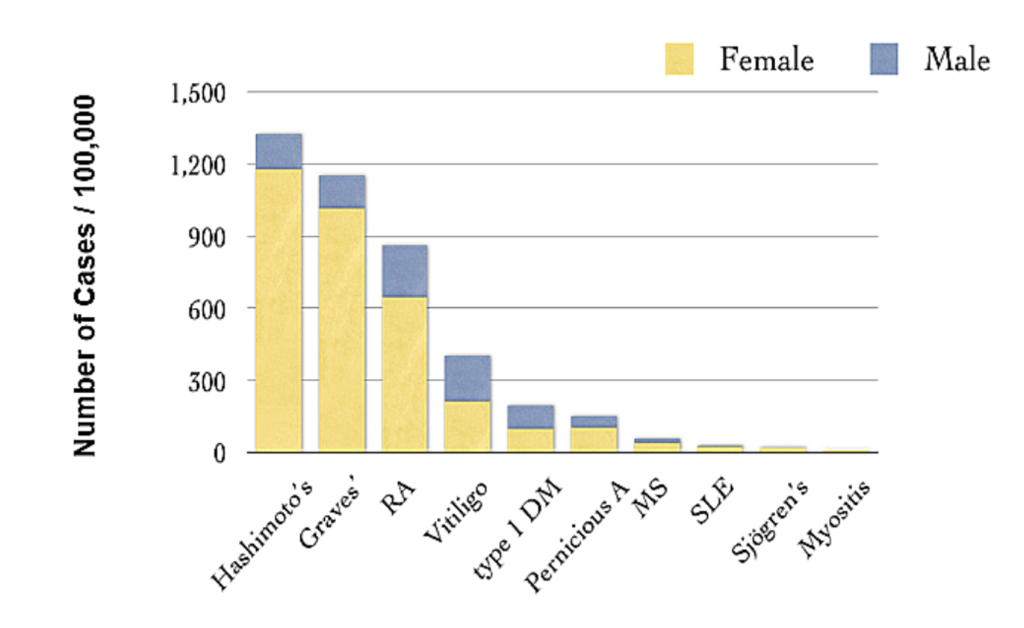
Johns Hopkins lists the top ten illnesses in the autoimmune disease category (below).
The distribution of autoimmune diseases varies from institution to institution or series to series in published literature. These illnesses may involve a single organ or multiple organs with local and/or systemic signs and symptoms.
A review of these ten conditions demonstrates the wide variation of autoimmune disease identified prior to the widespread use of mRNA products.
1 and 2. Thyroiditis: Autoimmunity can present as either thyroid underactivity, Hypothyroid (Hashimoto’s Disease) https://www.mayoclinic.org/diseases-conditions/hashimotos-disease/symptoms-causes/syc-20351855 or overactivity, Hyperthyroid (Graves’ Disease) (https://www.mayoclinic.org/diseases-conditions/graves-disease/symptoms-causes/syc-20356240). Autoimmune thyroiditis is an example of single organ disease with systemic symptoms.
3. Rheumatoid arthritis (RA): RA involves joints and supportive tissues with inflammation that can affect multiple joints and regions simultaneously. It is a debilitating disease. https://www.mayoclinic.org/diseases-conditions/rheumatoid-arthritis/symptoms-causes/syc-20353648.
Recall that the number one adverse event (AE) by system organ category (after “Other”) reported in Pfizer’s confidential post-marketing document 5.3.6, AEs from the first 10 weeks of emergency use inoculation of BNT162b2, was “Musculoskeletal.” (https://www.phmpt.org/wp-content/uploads/2022/04/reissue_5.3.6-postmarketing-experience.pdf) The data collection for that report ended on February 28, 2021.
Note that Autoimmune illness in the Pfizer data is number five.
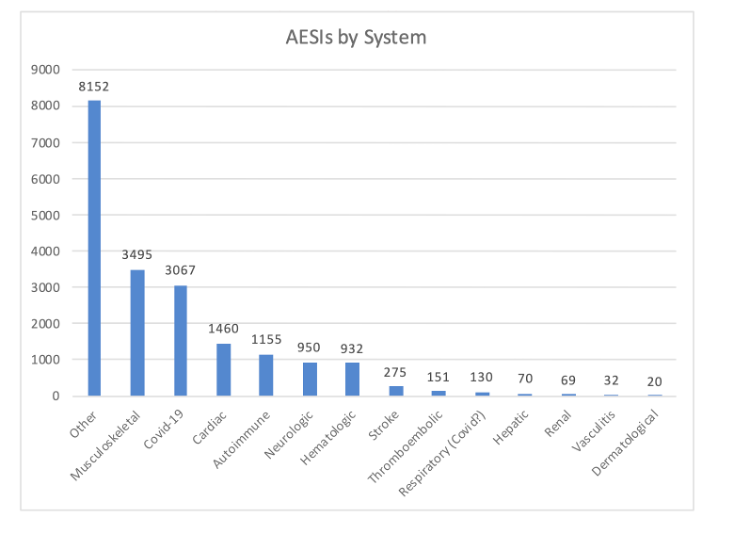
(https://dailyclout.io/pfizer-evidence-so-far-coverups-heart-damage-and-more/, p. 19 of PDF)
4. Vitiligo: A dermatologic condition. https://www.niams.nih.gov/health-topics/vitiligo
5. Type 1 diabetes is a result of autoimmune attack on insulin producing cells in the pancreas. https://www.cdc.gov/diabetes/basics/what-is-type-1-diabetes.html.
6. Pernicious anemia: Chronic anemia from reduced Vitamin B12 absorption. https://www.ncbi.nlm.nih.gov/books/NBK540989/
7. Multiple sclerosis: Demyelinating disease of the central nervous system. https://www.mayoclinic.org/diseases-conditions/multiple-sclerosis/symptoms-causes/syc-20350269
8. Systemic lupus erythematosus: Discussed below.
9. Sjogren’s syndrome: Involves salivary glands and musculoskeletal symptoms. https://www.ninds.nih.gov/health-information/disorders/sjogrens-syndrome
10. Myositis: Inflammation of muscles. https://www.hopkinsmyositis.org/myositis/
This topic was explored along with rhabdomyolysis in a previous report. https://dailyclout.io/report-67-part-4b-rhabdomyolysis-a-k-a-jellied-muscle-after-mrna-gene-therapy-injections/
Systemic Lupus Erythematosus
Signs and symptoms of autoimmune illness can vary over time and can manifest as multiorgan diseases such as Systemic Lupus Erythematosus, referred to as SLE or “Lupus.”
Lupus can appear with a diverse array of symptoms as reported by the Centers for Disease Control and Prevention (CDC). (https://www.cdc.gov/lupus/basics/symptoms.htm)
Lupus symptoms include:
- Muscle and joint pain. One may experience pain and stiffness, with or without swelling. This affects most people with lupus. Common areas for muscle pain and swelling include the neck, thighs, shoulders, and upper arms.
- A fever higher than 100 degrees Fahrenheit affects many people with lupus. The fever is often caused by inflammation or infection. Lupus medicine can help manage and prevent fever.
- One may get rashes on any part of the body that is exposed to the sun, such as face, arms, and hands. One common sign of lupus is a red, butterfly-shaped rash across the nose and cheeks.
- Chest pain. Lupus can trigger inflammation in the lining of the lungs. This causes chest pain when breathing deeply.
- Hair loss. Patchy or bald spots are common. Hair loss may also be caused by some medicines or infection.
- Sun or light sensitivity. Most people with lupus are sensitive to light, a condition called photosensitivity. Exposure to light can cause rashes, fever, fatigue, or joint pain in some people with lupus.
- Kidney problems. Half of people with lupus also have kidney problems, called lupus nephritis.3 Symptoms include weight gain, swollen ankles, high blood pressure, and decreased kidney function.
- Mouth sores. Also called ulcers, these sores usually appear on the roof of the mouth but can also appear on the gums, inside the cheeks, and on the lips. They may be painless, or one may have soreness or dry mouth.
- Prolonged or extreme fatigue. One may feel tired or exhausted even when getting enough sleep. Fatigue can also be a warning sign of a lupus flare.
- Fatigue can be a sign of anemia, a condition that happens when one’s body does not have red blood cells to carry oxygen throughout the body.
- Memory problems. Some people with lupus report problems with forgetfulness or confusion.
- Blood clotting. One may have a higher risk of blood clotting. This can cause blood clots in the legs or lungs, stroke, heart attack, or repeated miscarriages.
- Eye disease. One may get dry eyes, eye inflammation, and eyelid rashes.
Giant Cell Arteritis
GCA or Giant Cell Arteritis (a.k.a., Temporal Arteritis) is another autoimmune disease that commonly involves the temporal artery and can impair vision,
Giant cell arteritis is an inflammation of the lining of your arteries. Most often, it affects the arteries in your head, especially those in your temples. For this reason, giant cell arteritis is sometimes called temporal arteritis. (https://www.mayoclinic.org/diseases-conditions/giant-cell-arteritis/symptoms-causes/syc-20372758)
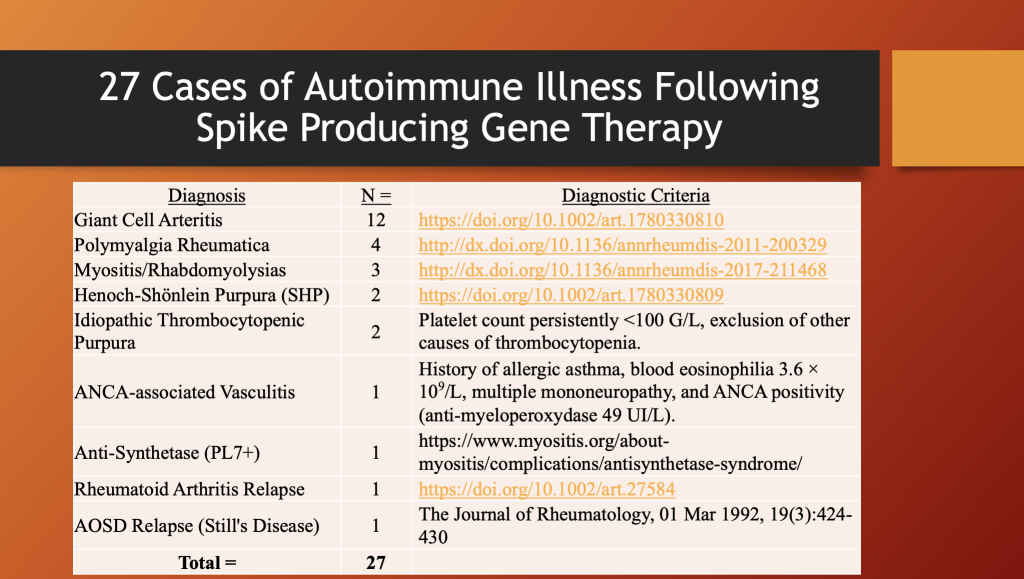
GCA was the leading autoimmune illness following COVID-19 gene therapy products in 27 patients in a study from Limoges, France, reported by Liozon, et al. [Liozon, E., et al. (Immune-Mediated Diseases Following COVID-19 Vaccination: Report of a Teaching Hospital-Based Case-Series. J. Clin. Med. 2022, 11, 7484.) https://doi.org/10.3390/jcm11247484.]
This paper is discussed in some detail later in this article.
The point being made here is the diversity and complexity of this very broad and heterogenous group of diseases can present both diagnostic and therapeutic challenges.
The graphic below illustrates some of the manifestations of autoimmunity.
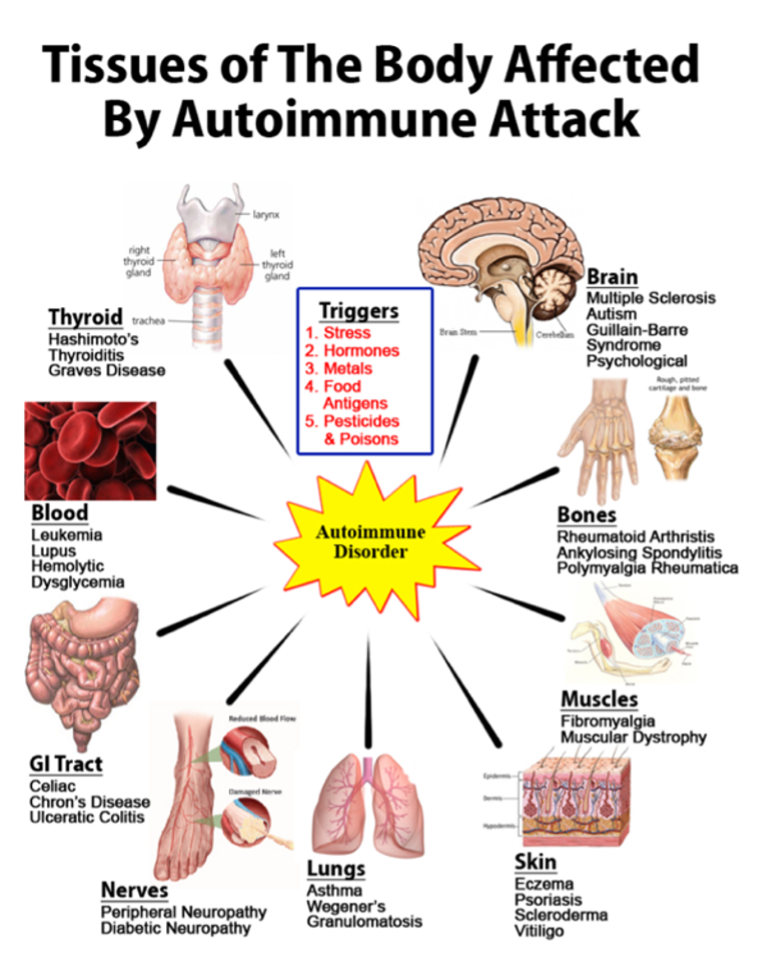
https://inimmune.com/wp-content/uploads/2016/05/Autoimmunity-768×995.png
{kind=link}
The Autoimmune Registry provides a list of autoimmune diseases with symptoms and links to additional references: https://www.autoimmuneregistry.org/the-list.
This article will not explore the complexities of autoimmune immunology, or the wide array of illnesses thought to be caused by this attack by self on self. Rather, it will explore the link between Spike-producing Gene Therapy drugs and autoimmune-like illnesses using a series report from France; case reports from Japan, Germany and Spain; and data and case reports from the Vaccine Adverse Events Reporting System (VAERS).
There will be some crossover between the subject of Part 4B in this series, Rhabdomyolysis (https://dailyclout.io/report-67-part-4b-rhabdomyolysis-a-k-a-jellied-muscle-after-mrna-gene-therapy-injections/), which has certain features of autoimmunity as well as Multisystem Inflammatory Syndrome in Children (MIS-C) featured in Histopathology Series Part 4D (in preparation) that concerns CoVax Disease in children, as well as this article on autoimmune disease. (The term CoVax Diseases (CVDs) is introduced here to describe the disease states associated with or are caused by injection of Spike-producing gene therapy products and encompass both pathologic processes based upon histopathologic analysis and clusters of illness conditions likely caused by lipid nanoparticle (LNP) components, synthetic mRNA, E.coli Kanamycin resistant DNA Plasmids, and Adenovirus-vectored DNA, and other Spike-producing drugs.)
II. Series Report
Liozon, et al. presented a series of 27 patients diagnosed with Immune-Mediated Diseases (IMDs) associated with use of Spike-generating drugs in a French referral hospital serving a population of 723,784. Data were collected during the period from January 2021 through May 31, 2022. (https://doi.org/10.3390/jcm11247484)
The authors are careful to point out that numerators and denominators cannot be measured or estimated, so incidence and prevalence statistics are not calculated.
Comparing the very limited crossover of this distribution with that from Johns Hopkins illustrates how varied these illnesses can be.
The 27 cases of autoimmune disease associated with Spike-producing drugs in this series are listed by category. Each category is listed with criteria used to make the diagnosis.
The discussion by the authors is interesting as the authors delicately handle the topic of safety.
“Phase-II trials have shown reassuring safety profiles in mRNA-based vaccines and viral vector-based vaccines.” (https://doi.org/10.3390/jcm11247484, p. 1.)
They go on to say caution is warranted because of “population wide surveys” have suggested “significant side effects.”
Nevertheless, recent safety data from population-wide surveys have suggested significant side effects, notably severe thrombotic events via vaccine-induced immune thrombotic thrombocytopenia. (https://doi.org/10.3390/jcm11247484, p. 1.)
The outcome for these patients was not favorable. Only 11% recovered, 60% well to poorly controlled on medications, one died, and 26% (7/27) were lost.
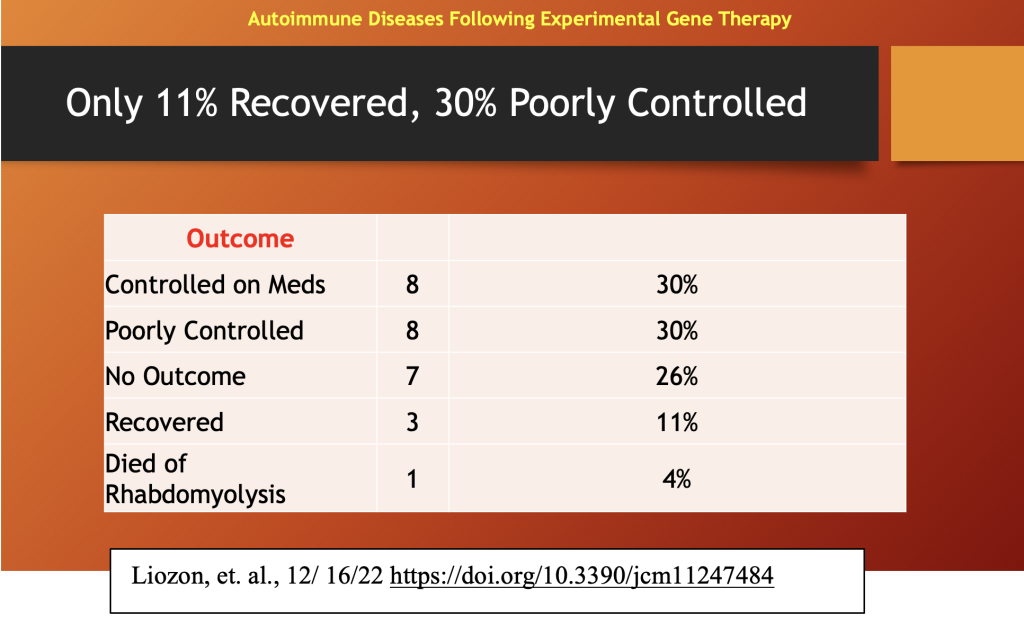
Treatment was not effective. Steroids were often the mainstay of treatment and were used in 93% (25/27) of the cases. Only three patients were “recovered.” Quotation marks are used as autoimmune illnesses can have periods of remission and reactivation. The positive ANA means that the disease is not gone.
Re-Inoculation after Autoimmune Disease Diagnosis: 11 patients
Remarkably, even when faced with the possibility of making the autoimmune condition worse, 11 patients were injected with up to three additional doses, “…without significant harm in 9…” (82%) which means two (18%) had significant harm that was not specified.
Final outcome after additional injections is given below for this subgroup. Limited data from 10 patients in this subgroup are given with no explanation of what happened to the eleventh patient.
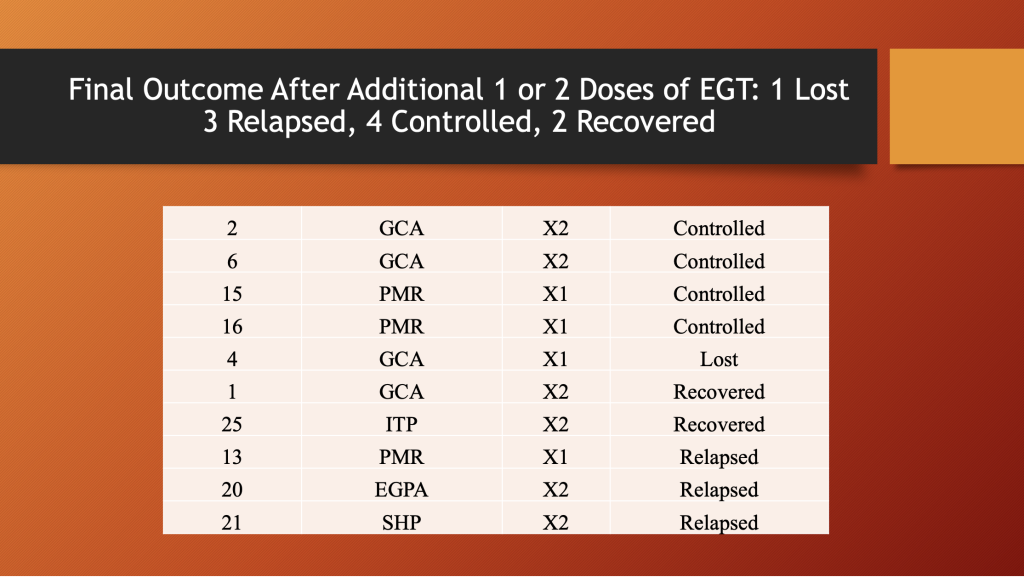
A third of these patients relapsed, 22% recovered, and 44% were chronically ill.
Conclusions: 27 patients
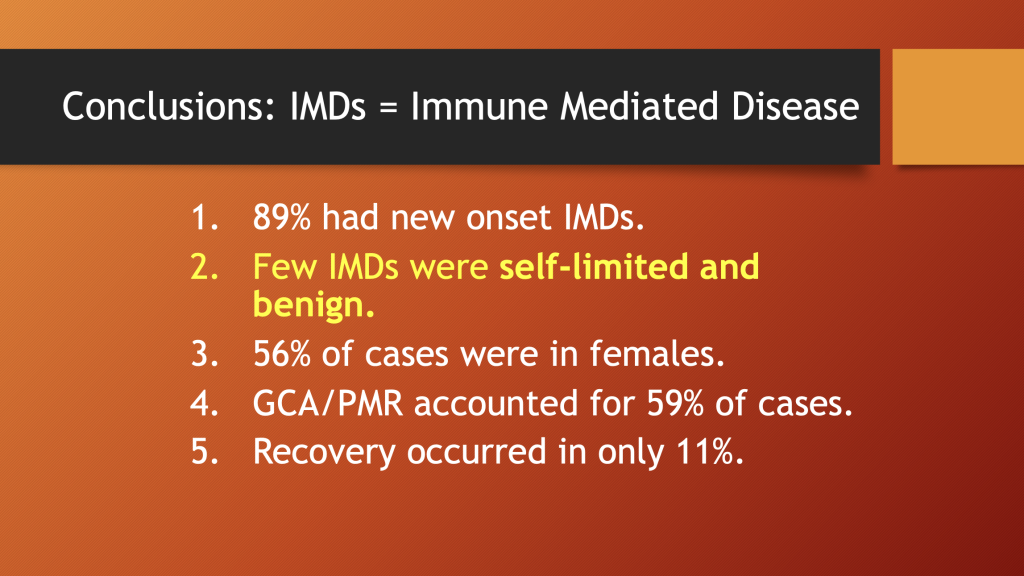
The authors concluded that 89% had new disease, and the rest were reactivation of pre-existing disease. Number two is in yellow to draw attention to the word choice used, “Few…were self-limited and benign.” The treatment records of these patients should be reviewed to understand the course of these illnesses, a key part of assessing the severity of a disease.
As with most data associated with the use of these products, the majority of cases occurred in women, 59% were Giant Cell arteritis or Polymyalgia Rheumatica, and only 11% were considered recovered.
Causation:
The authors present a confusing set of statements concerning the potential causal relationship between “vaccination” and Immune-Mediated Disease.
Here they say a causal relationship is “conjectural,” and, in the same sentence, they note that a flare from re-inoculation reinforced the hypothesis of causal relationship.
A causative relationship between vaccination and subsequent IMD is conjectural in the 27 patients, although rechallenge in two patients (Cases 1 and 20) resulted in a limited disease flare, reinforcing the hypothesis of a causal relationship between COVID-19 vaccination and GCA. (https://doi.org/10.3390/jcm11247484, p. 7.)
This is not the only example of what could be called forced ambiguity, because there are other examples of similar ambiguous phraseology.
Here they reinforce the notion that a causal relationship “…is not supported by our data” (emphasis added),
Therefore, a causal relationship between COVID-19 vaccination and subsequent IMDs is not supported by our data. (https://doi.org/10.3390/jcm11247484, p. 7.)
This is a clear statement of no causation between Spike therapies and IMDs.
Then in the next sentence,
Nevertheless, the strong temporal relationship between the two events raises legitimate safety concerns about COVID-19 vaccines in these patients. (https://doi.org/10.3390/jcm11247484, p. 7.)
The hedging continues,
Other cases of GCA or PMR temporally associated with COVID-19 vaccination have been published, suggesting the association to be not casual and that post-vaccine onset of GCA/PMR is not an exceptional occurrence. (Emphasis added.) (https://doi.org/10.3390/jcm11247484, p. 8.)
Now the association between the injection and IMDs is “…not casual…” Is this the same as saying causal? A lot hinges on which side of the “s” the “u” lands.
From our observations, unadjuvanted vaccines such as the currently marketed SARS-CoV-2 vaccines can induce GCA/PMR by acting as non specific triggers in genetically predisposed subjects (notably those with HLA-DRB1*04) possibly by strongly activating Toll-like receptor signaling. (Emphasis added.) ((https://doi.org/10.3390/jcm11247484, p. 9.)
Merriam-Webster Dictionary gives “cause” as a synonym for induce.
https://www.merriam-webster.com/dictionary/induce
The authors even supply a mechanism whereby the gene therapy drugs activate Toll-like receptors that lead to the disease states called IMDs.
Translation: SARS-CoV-2 “vaccines” cause IMDs or “light up” an underlying pre-existing IMDs with high enough probability to raise a safety signal. Why such tortured reasoning? Are the authors being watched?
III. Literature Clinical Pathological Case (CPC) Reports
Literature Case Report 1: 14-Year-Old with Eight Organs Involved
Fatality 45 hours after BNT162b2 Dose 3
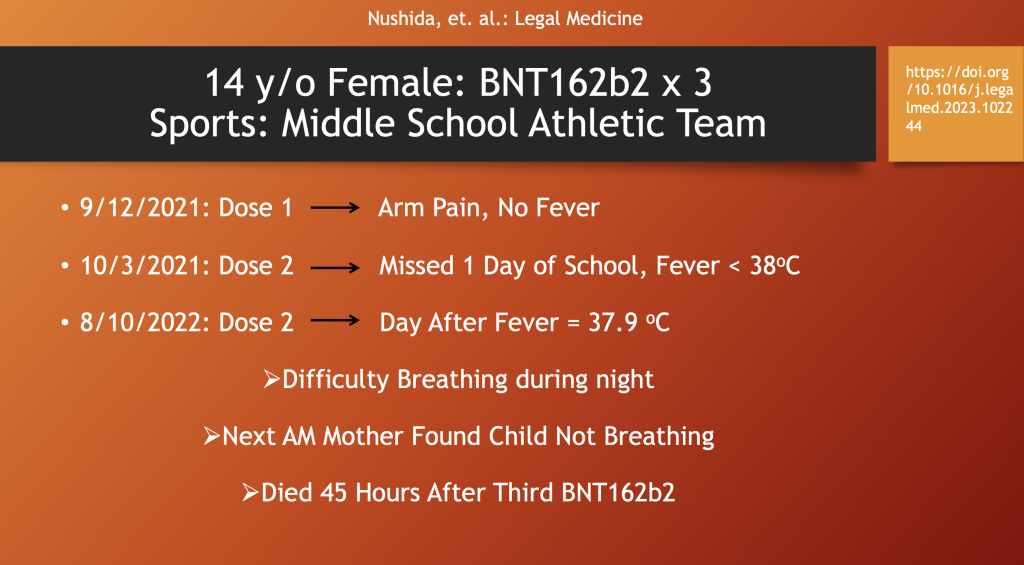
This case authored by Nushida, et al., comes from Tokushima, Japan, and tells the medical story of a healthy, 14-year-old, athletic girl who had the following chronology beginning with “reactogenicity” after her first two doses of BNT162b2 (arm pain, fever and malaise); then, 45 hours after her third dose, was found dead by her mother.
Her postmortem findings showed no evidence of virus.
Pertinent Negatives
- COVID-19 antigen quantification test: negative.
- Serum for adenovirus, cytomegalovirus, influenza virus (A, B), respiratory syncytial virus (RSV), Epstein-Barr virus, enterovirus (70, 71), parvovirus, and human immunodeficiency virus: negative
- Quantitative testing for the COVID-19 antigen using nasopharyngeal swabs yielded negative results.
- The results of polymerase chain reaction (PCR) tests performed for COVID-19 using swabs from the lung, heart, liver, kidney, stomach, duodenum, diaphragm, and cerebrum after formalin fixation were also negative.
- Blood at autopsy was tested for drug toxicity using LC-MS/MS, and the results were negative.
It is interesting that the authors did some blood tests and proclaimed there was no drug toxicity even after they concluded that the experimental drug she had been injected with three times was responsible for the child’s demise? Did they not consider the “vaccine” a drug? Is this an example of classical conditioning or perhaps a form of hypnosis.
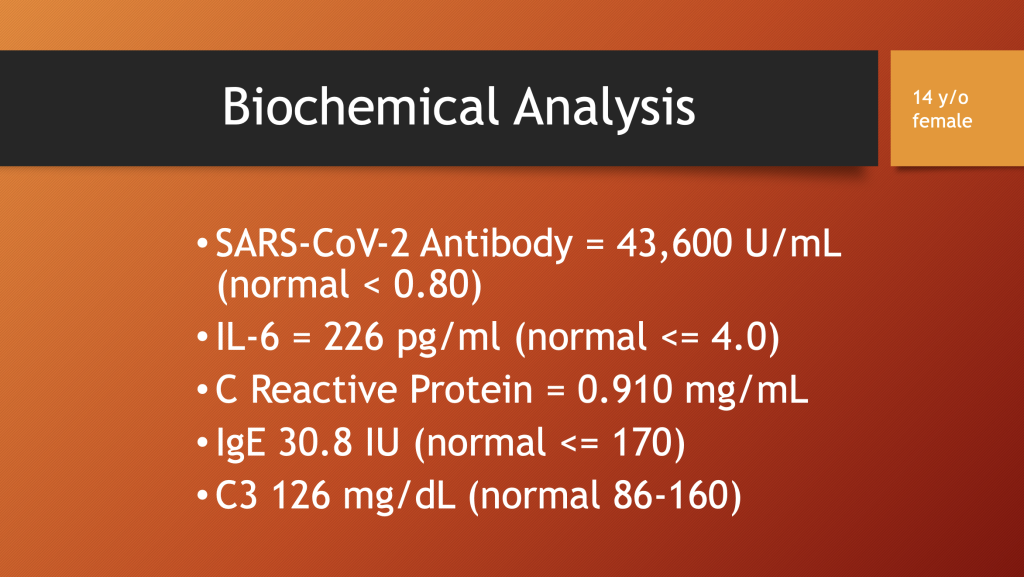
Biochemical Analysis
Presumably the SARS-CoV-2 antibody reported here was to Spike and not to nucleocapsid as the blood tests found no evidence of the virus past or present.
Elevated C Reactive Protein (CRP) and IL-6 are consistent with a systemic inflammatory reaction.
An autopsy was performed with the following gross findings. “Gross” refers to inspection with the naked eye.
At Autopsy: Gross Pathology Findings
- Heart: no degeneration or scarring on the grossly superficial surface or cross-sections.
- Lungs: showed severe pulmonary edema and
Histopathology with Special Stains
There are 24 histopathology sections from eight organs with three different stains indicating that the different organs attract different cell concentration and composition of activated white cells.
The viewer is dependent on the pathologist to present representative sections to indicate important findings. Sampling error should be taken into consideration.
Histopathology from eight organs shows infiltration with inflammatory lymphocytes.
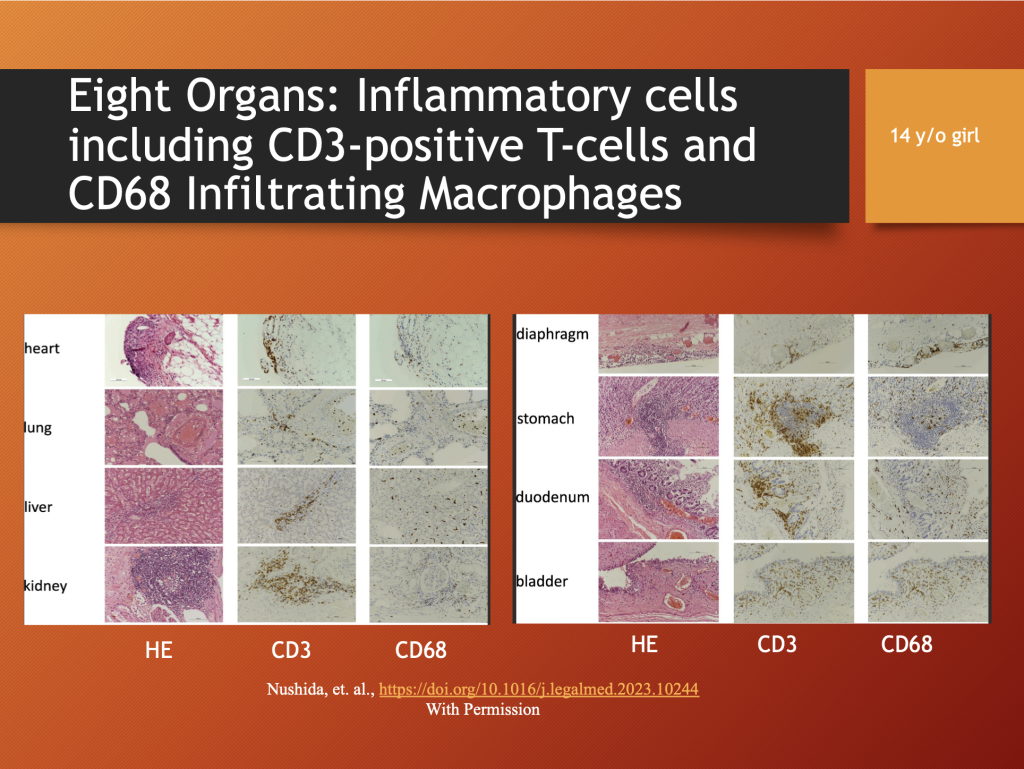
Fig. 1. Histopathology of the heart (left atrium), lung, liver, kidney, diaphragm, stomach, duodenum, and bladder. All images are × 200 magnification. HE: Hematoxylin and Eosin staining showing lymphocytic infiltration.
CD3: Immunohistochemical staining for CD3 showing inflammatory cells including CD3-positive T-cells. CD68: Immunohistochemical staining for CD68 shows the infiltrating cells include macrophages. (Used with permission).
The authors concluded (below) that the third dose of BNT162b2 produced a massive release of inflammatory chemicals from at least eight organs that was rapidly fatal. Like Turbocancer described by Dr. Burkhardt (https://dailyclout.io/report-58-part-2-autopsies-reveal-medical-atrocities-of-genetic-therapies-being-used-against-a-respiratory-virus/) and Dr. Krüger (https://dailyclout.io/report-61-ute-kruger-md-breast-cancer-specialist-reveals-increase-in-cancers-and-occurrences-of-turbo-cancers-following-genetic-therapy-vaccines/), Turboautoimmunity may be a diagnostic consideration.
Pay attention to #3 in the slide below. Common adverse reactions are characterized in the Pfizer documents, as well as publications in the medical literature, as “reactogenicity,” an industry invention that inhibits detailed follow-up to define whether there is an association between early reactions to vaccines and deleterious long-term medical problems.
Reactogenicity refers to a subset of reactions that occur soon after vaccination and are a physical manifestation of the inflammatory response to vaccination. In clinical trials, information on expected signs and symptoms after vaccination is actively sought (or ‘solicited’). These symptoms may include pain, redness, swelling or induration for injected vaccines, and systemic symptoms, such as fever, myalgia, headache, or rash. The broader term ‘safety’ profile refers to all adverse events (AEs) that could potentially be caused/triggered or worsened at any time after vaccination, and includes AEs, such as anaphylactic reactions, diseases diagnosed after vaccination and autoimmune events. (Emphasis added.) [https://www.nature.com/articles/s41541-019-0132-6 “The how’s and what’s of vaccine reactogenicity”, Herve, et al.www.nature.com/ npj/Vaccines, (2019)4:39.]
Case 1 Analysis
This case is not a typical autoimmunity case (See SLE below.) but rather is similar to the cytokine storm witnessed in patients with severe COVID-19. Catastrophic, multiorgan system failure with little advance warning is common to both conditions.
This presentation is also similar to Multisystem Inflammatory Syndrome in Children, MIS-C, or MIS-A in Adults. The rare condition known as Catastrophic Antiphospholipid Syndrome involves multiple organs but tends to occur in older females. (Cervera, Rodríguez-Pinto, Espinosa, Catastrophic Antiphospholipid Syndrome, Chapter 45 in Mosaic of Autoimmunity by Pericone and Schoenfeld, Academic Press, London, San Diego, Cambridge, Oxford, 2019. P484.)
The illness in this 14-year-old deceased may have a similar mass release of toxic substances from an autoimmune-mediated process resulting from successive doses of BNT162b2 and a final, mass event after a third presentation of Spike antigen following Dose 3.
The explanation for the mechanism producing the fatal outcome in this case offered by the authors in the conclusions above describes the terminal phase of this process, massive degranulation of lymphocytes.
The initial phase occurs when mRNA from BNT162b2 stimulates production of foreign proteins that draw a host reaction manifest as extensive infiltration of killer lymphocytes, C3 inflammatory cells, and C68 macrophages, as was seen in the histopathology from all eight organs of this young teenager. [https://www.abcam.com/primary-antibodies/human-cd-antigen-guide is a good source to identify the different antigens on leucocyte cell surfaces (CD or Cluster of Differentiation).]
BNT162b2 has known dose-related effects, and it is possible that each successive dose increases the magnitude of the cellular response. That cellular response consists of multiorgan infiltration of activated lymphocytes that suddenly and massively dump cytokines and other agents resulting in sudden death upon presentation of a third dose of BNT162b2. The terminal event may have been cardiac arrest.
Case 2: Literature Histopathology Series
Lymphocytic Infiltration and Muscle
Schwab, et al. presented histopathology from five cases of fatal myocarditis which they concluded were likely or possibly causally related to mRNA gene therapy products. (Schwab C, Domke LM, Hartmann L, Stenzinger A, Longerich T, Schirmacher P. Autopsy-based histopathological characterization of myocarditis after anti-SARS-CoV-2-vaccination. Clin Res Cardiol. 2023 Mar;112(3):431-440. doi: 10.1007/s00392-022-02129-5. Epub 2022 Nov 27. PMID: 36436002; PMCID: PMC9702955)
The authors provide the following schematic linking injected mRNA with CD4+ T cells and cardiac disease.
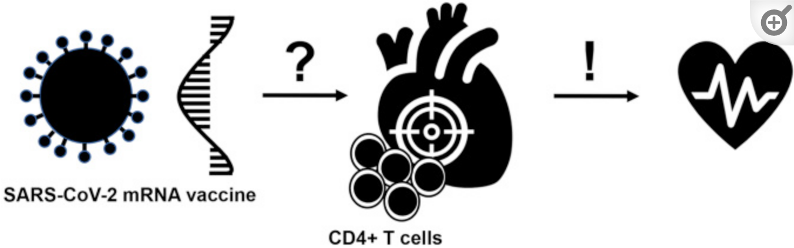
(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9702955/pdf/392_2022_Article_2129.pdf, p. 1)
Their findings were:
All cases showed a consistent phenotype: (A) focal interstitial lymphocytic myocardial infiltration, in three cases accompanied by demonstrable microfocal myocyte destruction. (B) T-cell dominant infiltrate with CD4 positive T-cells outnumbering CD8 positive T-cells by far; (C) frequently associated with T-cell infiltration of epicardium and subepicardial fat tissue revealing a similar immune phenotype (CD4 > > CD8). (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9702955/pdf/392_2022_Article_2129.pdf, p. 7.)
The inflammation observed in heart (smooth) muscle bears similarities with that seen in other muscle tissues following use of the gene therapy products.
The slide below is a compilation of histopathology from published or presented histopathology studies that share findings of lymphocytic infiltration in heart, deltoid, intestine, uterus, and aorta.
Lymphocytic Infiltration and Tissue Necrosis in Striated and Smooth muscle
Following C-19 Gene Therapy Products
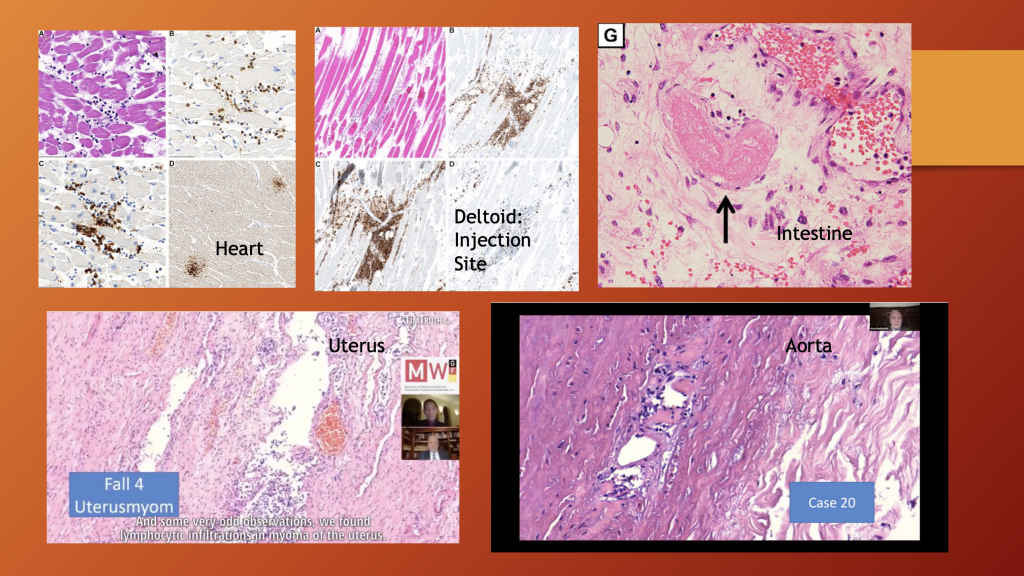
Top Left: Myocarditis Top Center: Myositis Deltoid (Schwab, et al.)
Top Right: Vasculitis Intestine, (Kamura, et al. Case 1)
Bottom Left: Uterus (Burkhardt Collection, https://dailyclout.io/report-58-part-2-autopsies-reveal-medical-atrocities-of-genetic-therapies-being-used-against-a-respiratory-virus/)
Bottom Right: Muscular Layer of Aorta (Burkhardt Collection, https://dailyclout.io/report-56-autopsies-reveal-the-medical-atrocities-of-genetic-therapies-being-used-against-a-respiratory-virus/)
Further analysis is necessary to understand more about lymphocyte activation and targeting in these cases.
The authors conclude by pointing to the uniqueness of the findings in autopsies on persons dying shortly after receiving Spike-Producing Gene Therapy Products compared with their past experience.
During the last 20 years of autopsy service at Heidelberg University Hospital we did not observe comparable myocardial inflammatory infiltration. This was validated by histological re-evaluation of age- and sex-matched cohorts from three independent periods, which did not reveal a single case showing a comparable cardiac pathology. (Emphasis added.) (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9702955/pdf/392_2022_Article_2129.pdf, p. 5.)
Case 2 Analysis
CoVax Diseases resemble their non-Spike implicated counterparts except in the severity and distribution of the former compared with the latter. Sudden death is not a common finding in non-Spike autoimmune disease.
Time will tell if there is some common pathomechanism in muscle tissues, both smooth and striated. The histopathology is similar in muscle tissue in the human body from aorta, to heart, to uterus, to intestine, to skeletal muscles. Rich vascularity is characteristic of smooth and striated muscle. Is the commonality vascularity or muscle? Or both?
Is the uterus responsible for the consistent predominance of women in having Adverse Events that has been identified in multiple LNP/mRNA data sets? In nine months, women can birth a seven- to eight-pound baby. Does this organ act like an LNP/mRNA magnet and Spike generator? Possibly.
Literature Case Report 3:
Systemic Lupus Erythematosus (SLE)
Lupus was introduced earlier in this article. Sogbe, et al. diagnosed a case of Systemic Lupus Erythematosus (SLE) in a 72-year-old woman with chronic renal failure from membranoproliferative glomerulonephritis (MPGN). [Sogbe, Miguel, et al. “Systemic Lupus Erythematosus Myocarditis after COVID-19 Vaccination.” Reumatología Clínica, Elsevier, 1 Feb. 2023, https://www.reumatologiaclinica.org/es-systemic-lupus-erythematosus-myocarditis-after-articulo-S1699258X22001553.]
Autoimmune disease had been ruled out before she was injected with BNT162b2.
The patient has been in chronic hemodialysis since 2017 after renal graft dysfunction due to chronic rejection. She presented to the emergency room with pleuritic chest pain one week after vaccination with the third dose of BNT162b2 mRNA. (https://www.reumatologiaclinica.org/es-systemic-lupus-erythematosus-myocarditis-after-articulo-S1699258X22001553)
Blood Studies (*Elevated):
- Haemoglobin 12.4 g/dl (12–16 g/dl),
- Total leucocyte count 4.86 × 10E9/L (4.8–10.8 × 10E9/L),
- Total lymphocyte count 0.58 × 10E9/L (1.2–4.5 × 10E9/L)*,
- Urea 91 mg/dl (16.6–48.5 mg/dl)*,
- Troponin I 231.5 ng/L (0–14 ng/L)* -peak value-,
- Erythrocyte sedimentation rate 17 mm/h (0–10 mm/h)*,
- C-reactive protein 0.58 mg/dl (≤0.5 mg/dl)*.
- SARS-CoV-2 PCR test was negative.
- Serological tests for cardiotropic pathogens were negative.
Autoimmune Serology:
- ANA (anti-nuclear antibody) IFA (indirect immunofluorescence assay) positive in 1:160 dilution*,
- Anti-dsDNA, and anti-histone antibodies were positive*,
- Low serum C3 level 75.50 mg/dl, (NV: 79–152 mg/dl)*,
- normal C4 level 27.50 mg/dl, (NV: 16–38 mg/dl) and
- normal CH50 level 537 U/ml, (NV: 392–1019 U/ml)
Her positive ANA IFA (indirect immunofluorescence assay), Anti-dsDNA, and anti-histone antibodies were essential to support the diagnosis of Lupus Myocarditis.
Diagnostic criteria for Lupus are given in the Appendix. Aringer, et al. provide the criteria for diagnosis used in the paper. [Aringer, Martin, et al. “2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus.” Wiley Online Library, Arthritis and Rheumatology, 6 Aug. 2019, https://onlinelibrary.wiley.com/doi/10.1002/art.40930.]
She was successfully treated with prednisone and beta-blockers. At follow-up three months after discharge, she appeared to be in remission but with positive serology indicating a potential for recurrent illness.
The authors implicate injected mRNA as the cause of her cardiac disease.
Case 3 Analysis
What sets this case apart is the clear serologic evidence of systemic lupus erythematosus (SLE). In spite of many morbidities, she responded to steroids and a medication to control her heart rate.
This individual might have had a subclinical case of systemic lupus erythematosus that was brought out by BNT162b2. Alternatively, the drug might have been the sole cause of her SLE.
IV. VAERS Data 2000-2022: Reports of Autoimmunity
There was a 24-fold increase in reported cases of autoimmunity in VAERS going from only COVID-19 disease in 2020 to COVID-19 gene therapy injections and COVID-19 in 2021. The reporting then dropped off precipitously in 2022.
Fatalities associated with these reported cases of autoimmunity averaged 0.4 per year for the two decades prior to the rollout of the COVID-19 gene therapy products before they jumped 37-fold, to 15, in 2021.
VAERS Case 1: Autoimmune MIS-C
Previously Healthy 12-Year-Old Male
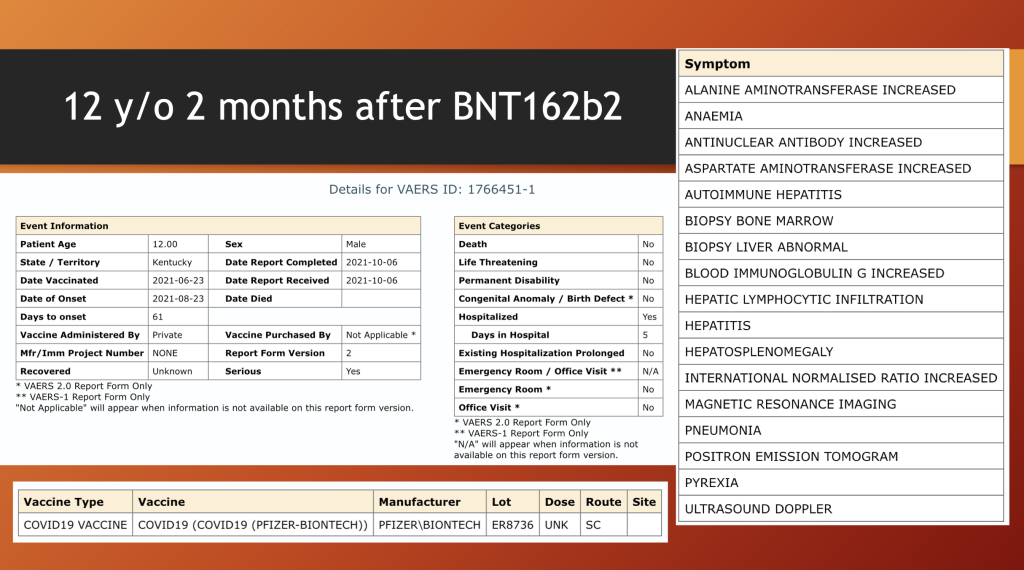
This 12-year-old boy spent five days in the hospital with multiple organ involvement including anemia, hepatitis, pneumonia, lymphoblastic hepatic infiltrate, and an enlarged spleen following BNT162b2 injection. The brief entry in VAERS included the comment that this presentation of autoimmune hepatitis was unusual.
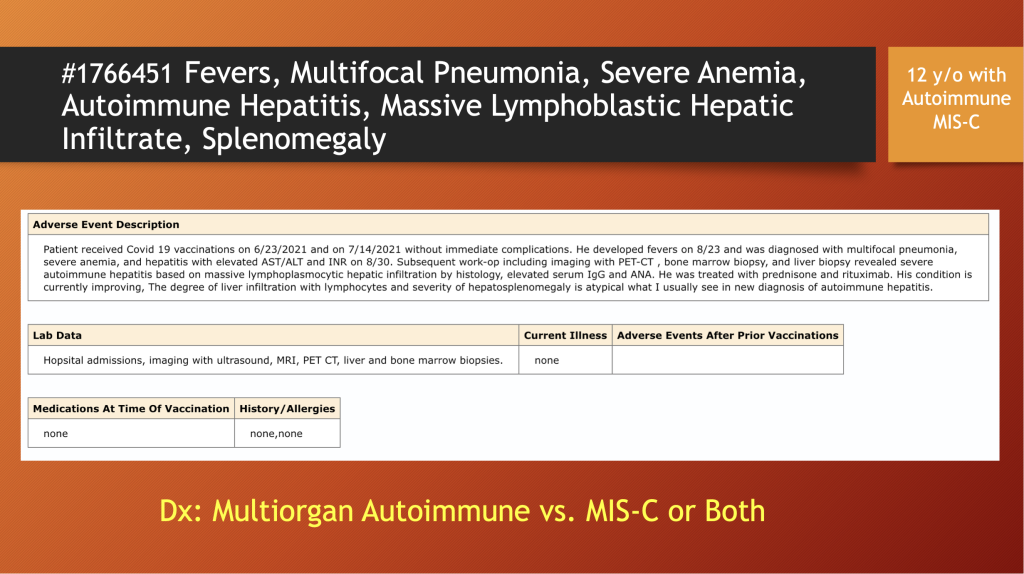
“The degree of liver infiltration with lymphocytes and severity of hepatosplenomegaly is atypical for what I usually see in new diagnosis of autoimmune hepatitis.”
Unfortunately, the information contained in this entry was limited, and the histopathology findings were not reported.
He was hospitalized for five days and had an extensive medical workup including liver and bone biopsies, MRI, and PET scans. His ANA was positive like the last case. More information would be helpful, but VAERS is a Registry and not a detailed medical record.
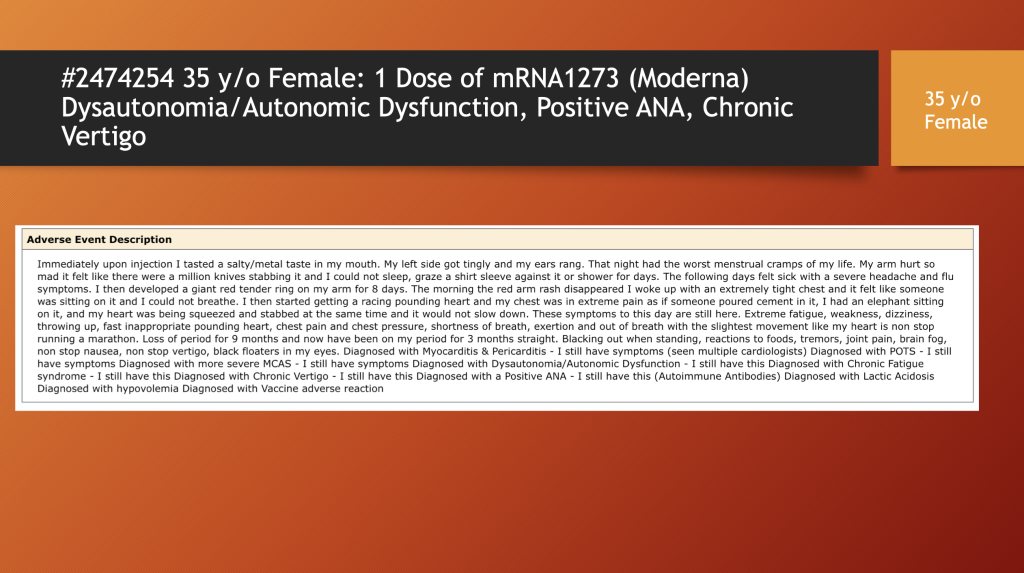
VAERS Case 2: Positive ANA, Vestibular Dysfunction, Myocarditis,
Chronic Fatigue, Menstrual Dysfunction…Permanent Disability
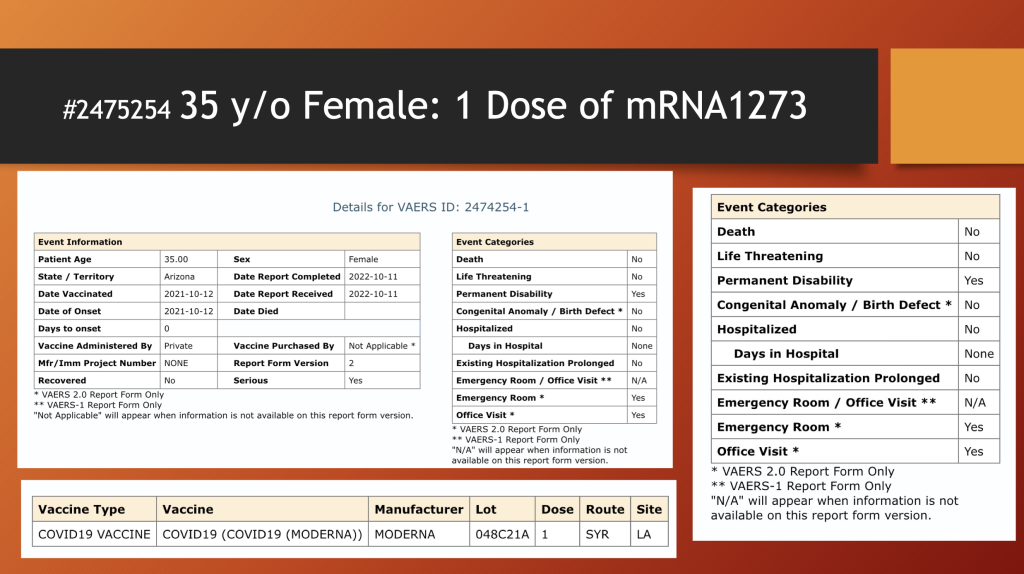
The 35-year-old woman had loss of her period for nine months, and then she reported having had a period lasting three months. Her symptoms began the day she was injected.
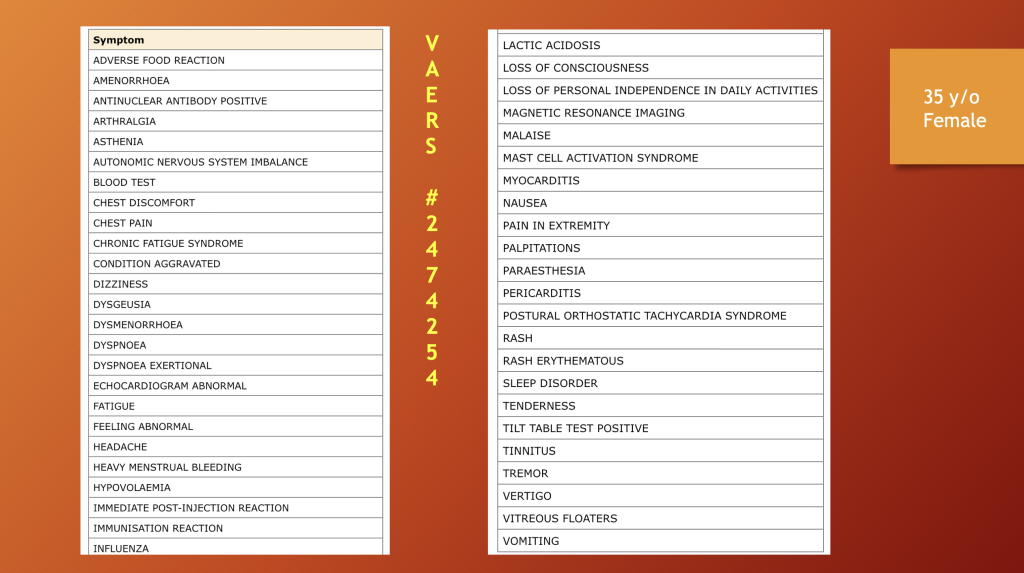
She had an extensive problem list with multiple organ system representation. Her ANA titers were elevated.
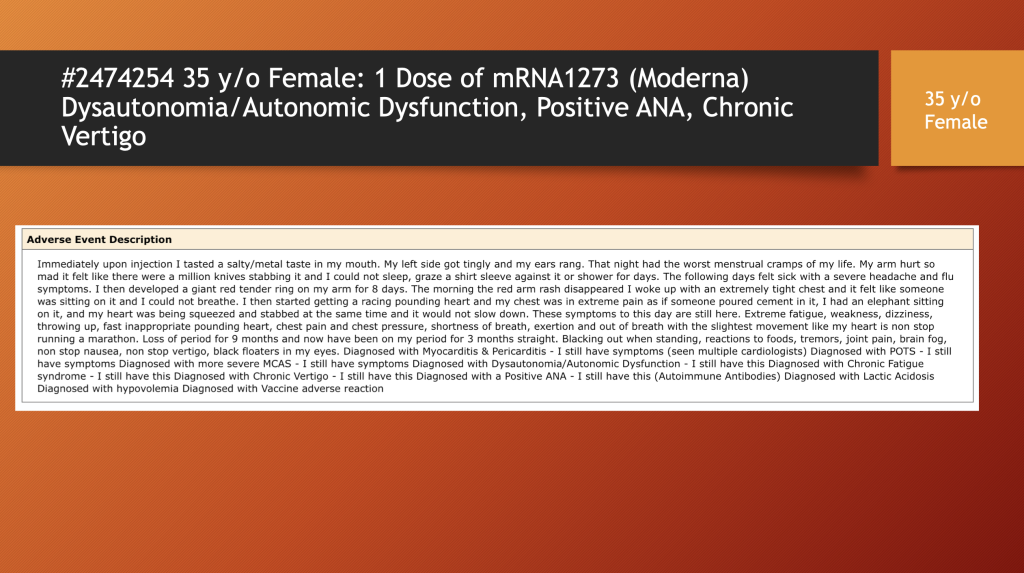
She reported she was left with permanent disability one year after the onset of her illness.
VAERS Case 3:
29-Year-Old Female with Central and Peripheral Nervous System Dysfunction and Peri-Myocarditis…Permanent Disability
This 29-year-old woman received one dose of BNT162b2 followed 12 days later by numerous adverse events, including cardiac and neurological problems that required three days of hospitalization.
She reported central and peripheral nervous system involvement as well as peri-myocarditis and arrhythmia.
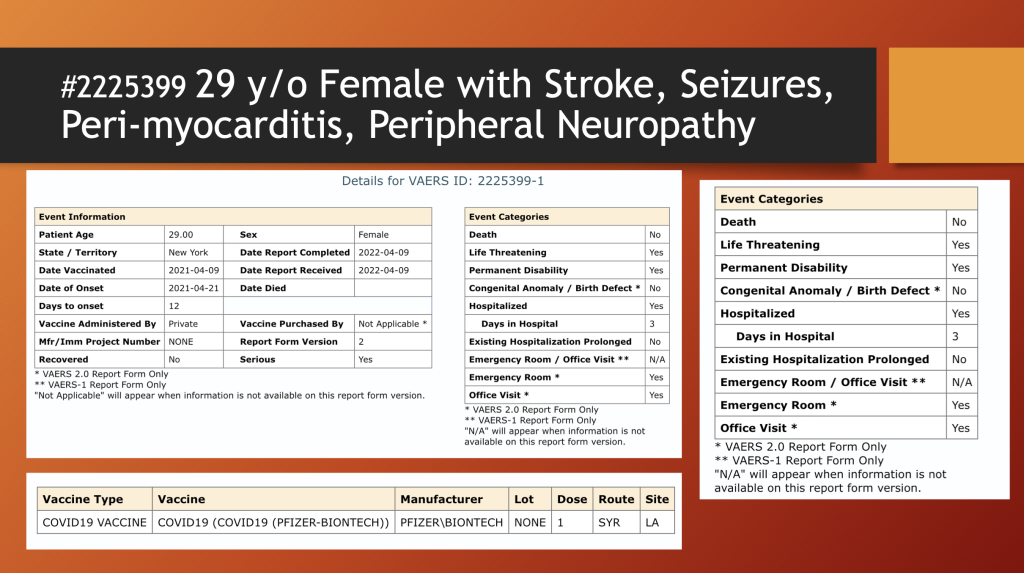
A year later, she was receiving ongoing treatment. She reported that she was permanently disabled. A 29-year-old with rapid onset of hormonal, cardiac, neurologic, and vascular disease is stunning.
V. Mechanism of Injury
BNT162b2 and mRNA1273, Moderna’s mRNA COVID “vaccine,” are complicated products designed to be delivered throughout the human body, including crossing the blood-brain barrier and placental barrier.
Adverse events can potentially be related to five components of these drugs: the whole preparation upon delivery into the deltoid, the lipid coating, the mRNA, Spike and related proteins produced by the mRNA, and E. coli plasmid contamination. Autoimmunity most likely comes from foreign proteins translated from the injected synthetic mRNA (#3 and #4).
![]()
The inset diagram above illustrates how the mRNA component may cause autoimmune disease. [This schematic was presented by Dr. Michael Palmer, MD on Children’s Health Defense TV on April 28, 2023, and is used with permission. (https://live.childrenshealthdefense.org/chd-tv/shows/friday-roundtable/components-of-mrna-vaccines-a-scientific-analysis/)]
The lipid nanoparticle (LNP) vehicle delivers mRNA to cells. mRNA is then released and commandeers the host’s cellular machinery to produce Spike and related proteins. These proteins are then recognized by the host immune system as foreign or not self. The host then launches an immune attack to destroy cells and extracellular material containing non-self-antigens causing an inflammatory reaction as well as associated tissue damage and clinical signs and symptoms.
VI. Discussion:
Conspicuously absent from the medical literature are large series reports of inflammatory conditions following injection of novel gene therapies for COVID-19. This includes the final report of the two-year findings of the original Phase 2/3 Clinical Trial of over 40,000 subjects which, unfortunately, was unblinded, thus ending the control group.
No prospective studies are in evidence, and there are few retrospective studies in spite of the fact that Pfizer confidential document 5.3.6 identified autoimmunity associated with the use of its LNP/mRNA product following widespread use of this product under the Emergency Use Authorization (EUA) granted by the Food and Drug Administration (FDA) in December 2020 until data collection for 5.3.6 ended on February 28, 2021.
Case reports, small autopsy series, and a small clinical series have documented a wide array of autoimmune illnesses ranging from limited organ involvement, such as Giant Cell Arteritis, to severe, sometimes catastrophic, cascading progressive multiple organ failure involving skin, brain, peripheral nervous system, liver, spleen, kidney, smooth and striated muscle, heart, intestines, uterus, testes, blood vessels, and skeletal muscle.
Polykretis, et al. published a paper March 8, 2023, in which they reviewed current evidence linking autoimmunity and COVID-19 genetic vaccines. (doi:10.20944/preprints202303.0140.v1)
They concluded:
- Autoimmunity is a central flaw in the mRNA platform. Genetic vaccines instruct human cells to manufacture viral protein in order to obtain an immune response, thereby producing an autoimmune response in organs.
- Prolonged persistence of mRNA in circulation and tissues maintains exposure to mRNA longer than the advertised few days.
- Adequate biodistribution studies were not performed before widespread inoculation of billions of people. Polykretis, et al. cite studies showing persistence of synthetic mRNA in blood for two weeks and persistence in lymph nodes up to eight weeks.
- Exosomes (https://www.annualreviews.org/doi/pdf/10.1146/annurev-biochem-013118-111902) are small transport vehicles that can distribute intact mRNA throughout the body by the vascular and lymphatic systems and illustrate possible distribution from origin in the spleen to heart, liver, and brain.
- Strong histological evidence supports COVID-19 vaccine-induced inflammation in tissues from T-lymphocytic infiltration.
VII. Conclusions
This review presents clinical evidence in support of the hypothesis that autoimmunity is one of the principal pathological mechanisms of harm from COVID-19 gene therapy drugs and, as such, represents a central flaw in the LNP/mRNA platform.
VAERS reporting of autoimmunity cases jumped from 35 in COVID-19 year one, 2020, to 840 in year one of the COVID-19 gene therapy products —a 24x increase in reports and a 37x increase in annual fatalities.
Incompletely tested, novel gene therapy is now associated with protean disease manifestations that derive from widespread biodistribution of products that enter host cells and translate mRNA code into Spike proteins that the host immune system has never seen.
Foreign proteins call forth an immune response from the host that target and destroy Spike proteins in host tissues and organs, sometimes dramatically and fatally.
The widespread organ involvement and severity of illness warrant consideration of a new class of illness, CoVax Disease, encompassing multiple pathological mechanisms of which autoimmunity occupies a central position.
Clotting and vascular disorders, neurological disease, direct toxicity, and neoplasia should also be considered part of this collection of harms following LNP/mRNA therapy at this early stage in the study of these disorders.
Appendix: SLE
The difficulty in recognizing many of the autoimmune diseases is illustrated well by the disease called systemic lupus erythematosus. The complexity criteria developed by the combined European League Against Rheumatism and the American College of Rheumatology points to the diagnostic challenge these illnesses present, not to mention the task of developing effective treatments.
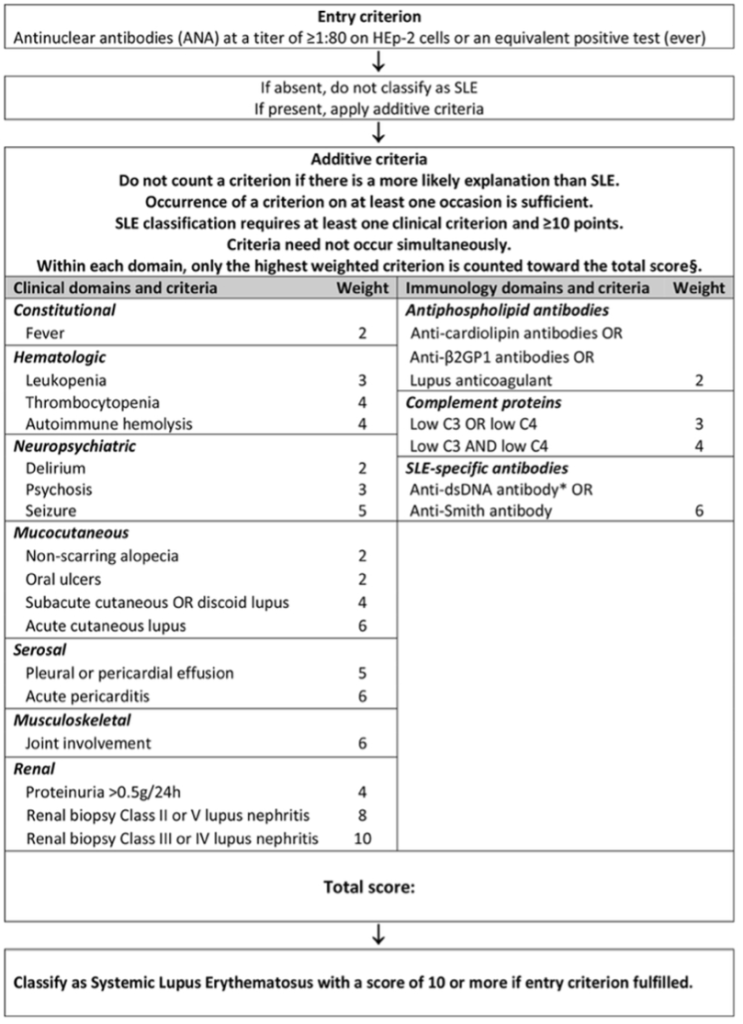
https://onlinelibrary.wiley.com/doi/10.1002/art.40930